

Tumor cells can follow distinct evolutionary paths to become resistant to epidermal growth factor receptor inhibition
- PMID: 26828195
- PMCID: PMC4900892
- DOI: 10.1038/nm.4040
Tumor cells can follow distinct evolutionary paths to become resistant to epidermal growth factor receptor inhibition
Abstract
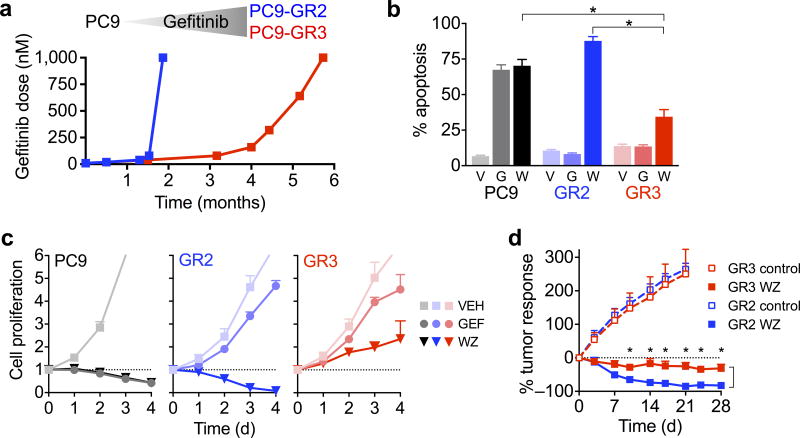
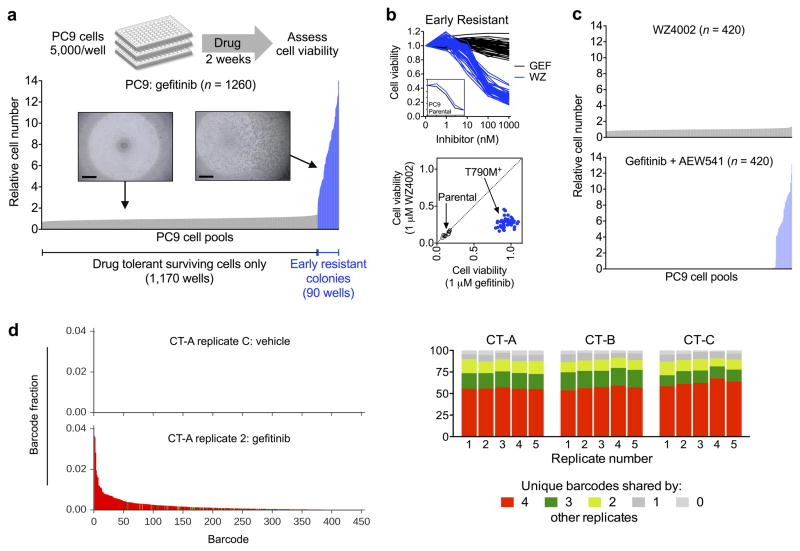
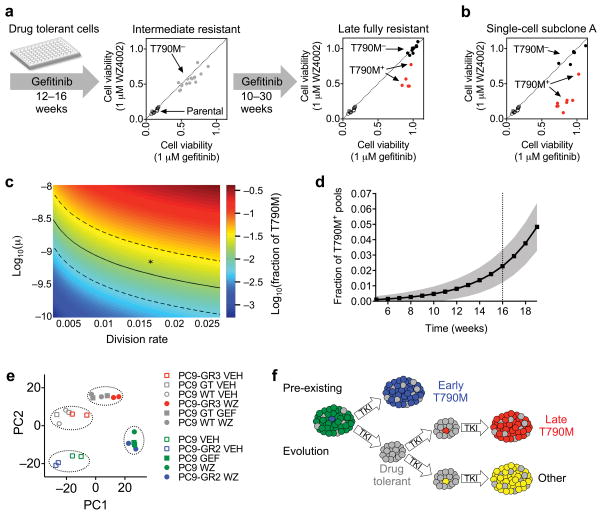
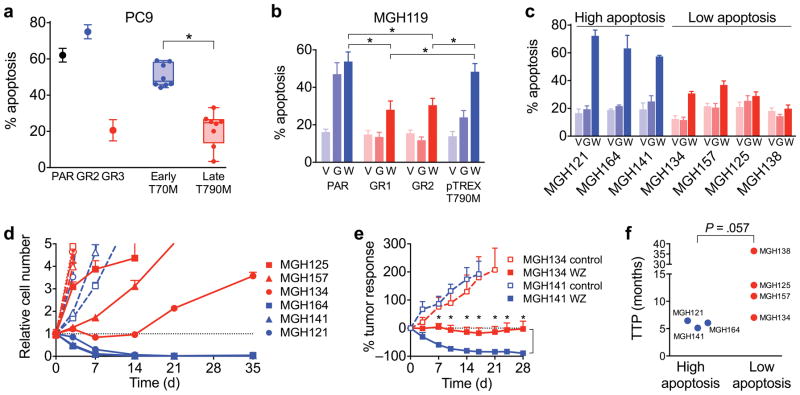
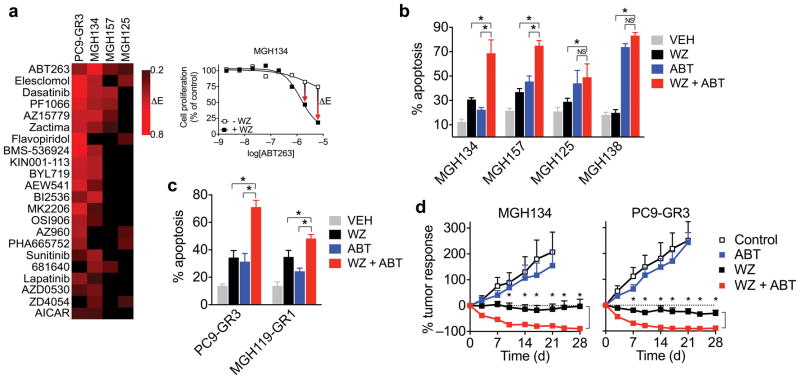
Although mechanisms of acquired resistance of epidermal growth factor receptor (EGFR)-mutant non-small-cell lung cancers to EGFR inhibitors have been identified, little is known about how resistant clones evolve during drug therapy. Here we observe that acquired resistance caused by the EGFR(T790M) gatekeeper mutation can occur either by selection of pre-existing EGFR(T790M)-positive clones or via genetic evolution of initially EGFR(T790M)-negative drug-tolerant cells. The path to resistance impacts the biology of the resistant clone, as those that evolved from drug-tolerant cells had a diminished apoptotic response to third-generation EGFR inhibitors that target EGFR(T790M); treatment with navitoclax, an inhibitor of the anti-apoptotic factors BCL-xL and BCL-2 restored sensitivity. We corroborated these findings using cultures derived directly from EGFR inhibitor-resistant patient tumors. These findings provide evidence that clinically relevant drug-resistant cancer cells can both pre-exist and evolve from drug-tolerant cells, and they point to therapeutic opportunities to prevent or overcome resistance in the clinic.
Conflict of interest statement
The authors declare competing financial interests: J.A.E. is a consultant for Novartis, Sanofi, Genentech, Clovis and Astra Zeneca; owns equity in Gatekeeper Pharmaceuticals, which has interest in T790M inhibitors; has research agreements with Novartis and Astra Zeneca. A.N.H. has provided consulting services for Amgen. M.J.N. has provided consulting services for Boehringer-Ingelheim. Z.P. has provided consulting services for Clovis Oncology and Boehringer-Ingelheim. L.V.S. has provided uncompensated consulting services to Clovis Oncology, AstraZeneca, Novartis, Boehringer-Ingelheim, Merrimack Pharmaceuticals, Genentech and Taiho Pharmaceuticals. H.C.B., V.K.R., C.L.K, D.A.R and and F.S. are employees of Novartis, Inc., as noted in the affiliations.
Figures
Comment in
-
Resistance: Following different paths.Nat Rev Cancer. 2016 Mar;16(3):128. doi: 10.1038/nrc.2016.23. Nat Rev Cancer. 2016. PMID: 26911183 No abstract available.
References
-
- Mok T, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361:947–957. - PubMed
-
- Maemondo M, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010;362:2380–2388. - PubMed
-
- Camidge DR, Pao W, Sequist LV. Acquired resistance to TKIs in solid tumours: learning from lung cancer. Nat Rev Clin Oncol. 2014;11:473–481. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
