

Partial restoration of the microbiota of cesarean-born infants via vaginal microbial transfer
- PMID: 26828196
- PMCID: PMC5062956
- DOI: 10.1038/nm.4039
Partial restoration of the microbiota of cesarean-born infants via vaginal microbial transfer
Abstract
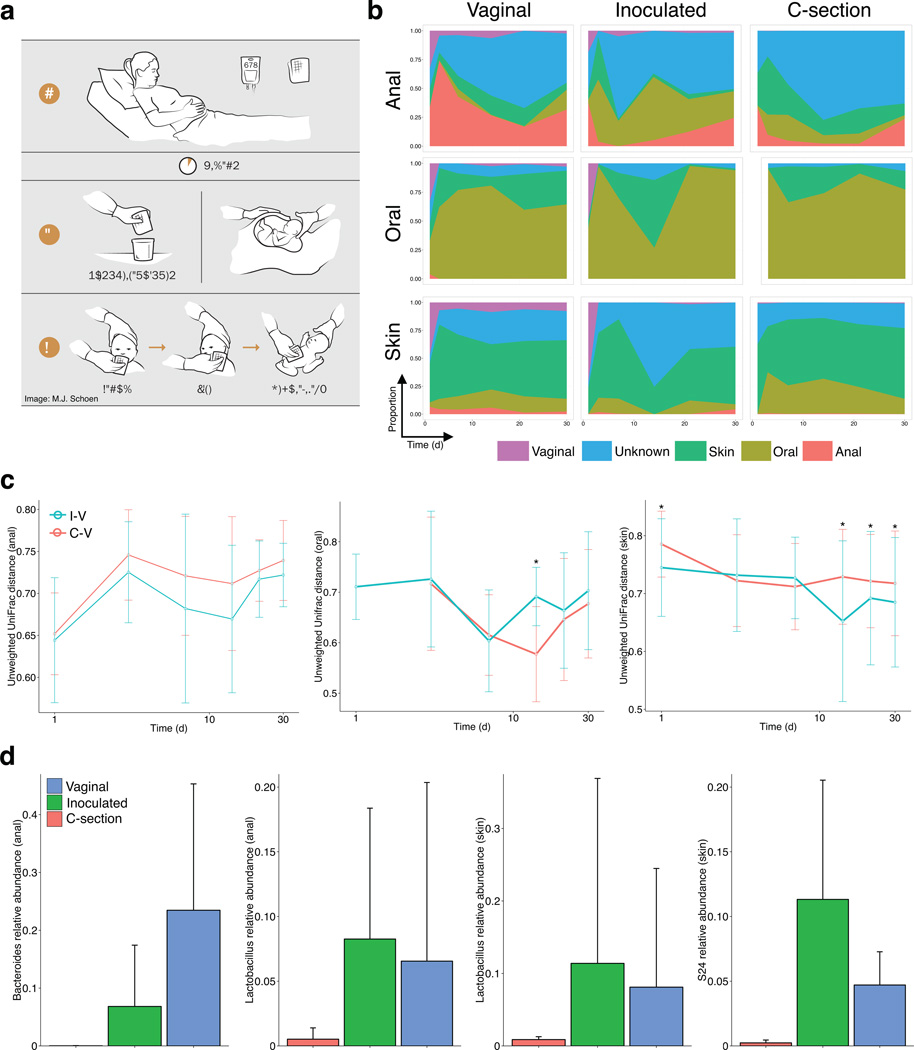
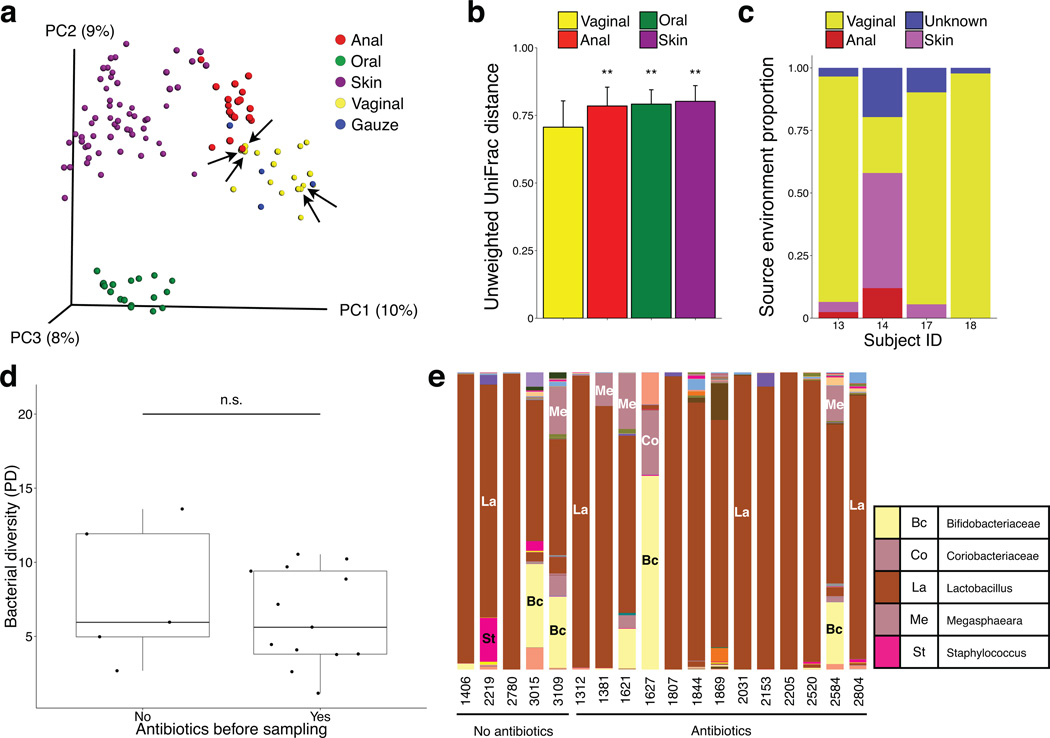
Exposure of newborns to the maternal vaginal microbiota is interrupted with cesarean birthing. Babies delivered by cesarean section (C-section) acquire a microbiota that differs from that of vaginally delivered infants, and C-section delivery has been associated with increased risk for immune and metabolic disorders. Here we conducted a pilot study in which infants delivered by C-section were exposed to maternal vaginal fluids at birth. Similarly to vaginally delivered babies, the gut, oral and skin bacterial communities of these newborns during the first 30 d of life was enriched in vaginal bacteria--which were underrepresented in unexposed C-section-delivered infants--and the microbiome similarity to those of vaginally delivered infants was greater in oral and skin samples than in anal samples. Although the long-term health consequences of restoring the microbiota of C-section-delivered infants remain unclear, our results demonstrate that vaginal microbes can be partially restored at birth in C-section-delivered babies.
Figures
Comment in
-
First microbial encounters.Nat Med. 2016 Mar;22(3):231-2. doi: 10.1038/nm.4042. Epub 2016 Feb 1. Nat Med. 2016. PMID: 26828194 No abstract available.
References
-
- Thavagnanam S, Fleming J, Bromley A, Shields MD, Cardwell CR. A meta-analysis of the association between Caesarean section and childhood asthma. Clinical and experimental allergy : journal of the British Society for Allergy and Clinical Immunology. 2008;38:629–633. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
