

A Retrospective Analysis of the Impact of Myomectomy on Survival in Uterine Sarcoma
- PMID: 26828206
- PMCID: PMC4735478
- DOI: 10.1371/journal.pone.0148050
A Retrospective Analysis of the Impact of Myomectomy on Survival in Uterine Sarcoma
Erratum in
-
Correction: A Retrospective Analysis of the Impact of Myomectomy on Survival in Uterine Sarcoma.PLoS One. 2016 Apr 14;11(4):e0153996. doi: 10.1371/journal.pone.0153996. eCollection 2016. PLoS One. 2016. PMID: 27078148 Free PMC article. No abstract available.
Abstract
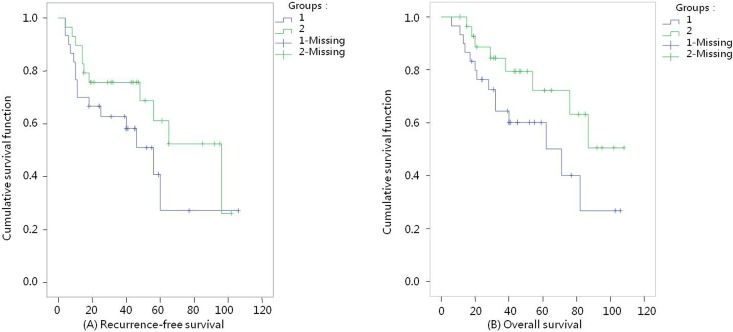
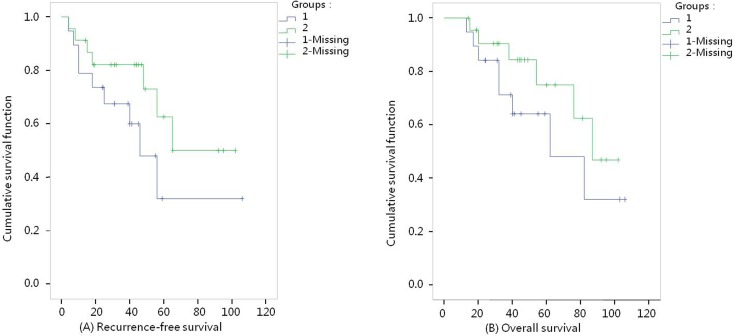
Laparoscopic myomectomy is a minimally invasive, conservative surgical approach commonly used for the treatment of uterine fibroids. However, there is a lack of effective means to distinguish the nature of uterine tumors prior to surgery. The impact of fibroid morcellation during laparoscopic surgery on the dissemination of cancerous uterine fibroids and long-term survival of patients has gained increasing attention. A retrospective cohort study was conducted to analyze the impact of different surgical approaches on recurrence-free survival (RFS) and overall survival (OS) in patients with a postoperative pathological diagnosis of uterine sarcoma at a single medical center. Patients who underwent the first surgery for uterine fibroids (confined to the uterus) and had a postoperative pathological diagnosis of uterine sarcoma were selected in the Chinese PLA General Hospital from January 2005 to January 2014. Based on the use of fibroid morcellation, the subjects were divided into fibroid morcellation (FM) and total hysterectomy (TH, non-morcellation) groups. Follow-up outcomes, including RFS and OS times, were observed. In total, 59 patients were included, with 30 cases in the FM group and 29 cases in the TH group. There were no significant differences in RFS and OS time between the two groups (RFS: P = 0.16, OS: P = 0.09). Multivariate correlation analysis showed that the impact of a higher grade level on RFS and OS was nearly 2-fold the impact of a lower grade level (RFS: P = 0.04, odds ratio (OR) = 1.97; OS: P = 0.03, OR = 2.29). Intraoperative morcellation, postoperative adjuvant therapy, age, tumor size, FIGO stage, and surgical approach were not risk factors affecting RFS and OS. Fibroid morcellation during laparoscopic surgery (including laparoscopic, transvaginal and transabdominal approaches) had no significant impact on RFS and OS time in patients. However, the 5-year RFS and OS rates were both lower in the FM group than in the TH group. Grade level was a significant risk factor for the prognosis of patients with uterine sarcoma.
Conflict of interest statement
Figures
Similar articles
-
The impact of tumor morcellation during surgery on the prognosis of patients with apparently early uterine leiomyosarcoma.Gynecol Oncol. 2011 Aug;122(2):255-9. doi: 10.1016/j.ygyno.2011.04.021. Epub 2011 May 12. Gynecol Oncol. 2011. PMID: 21565389
-
A Multicentre Retrospective Review of Clinical Characteristics of Uterine Sarcoma.J Obstet Gynaecol Can. 2017 Aug;39(8):652-658. doi: 10.1016/j.jogc.2017.03.090. J Obstet Gynaecol Can. 2017. PMID: 28729098
-
Uterine sarcomas and parasitic myomas after laparoscopic hysterectomy with power morcellation.Am J Obstet Gynecol. 2015 May;212(5):594.e1-10. doi: 10.1016/j.ajog.2014.12.002. Epub 2014 Dec 11. Am J Obstet Gynecol. 2015. PMID: 25499259
-
Laparoscopic power morcellation of presumed fibroids.Minerva Ginecol. 2016 Jun;68(3):352-63. Epub 2016 Jan 22. Minerva Ginecol. 2016. PMID: 26799759 Review.
-
Morcellation of occulted sarcomas during laparoscopic myomectomy and hysterectomy for patients with large fibroid uterus.Minerva Ginecol. 2018 Feb;70(1):84-88. doi: 10.23736/S0026-4784.17.04149-1. Epub 2017 Oct 3. Minerva Ginecol. 2018. PMID: 28975775 Review.
Cited by
-
Sarcoma of the Uterus. Guideline of the DGGG and OEGGG (S2k Level, AWMF Register Number 015/074, February 2019).Geburtshilfe Frauenheilkd. 2019 Oct;79(10):1043-1060. doi: 10.1055/a-0882-4116. Epub 2019 Oct 22. Geburtshilfe Frauenheilkd. 2019. PMID: 31656317 Free PMC article.
-
Sarcoma of the Uterus. Guideline of the DGGG, OEGGG and SGGG (S2k-Level, AWMF Registry No. 015/074, April 2021).Geburtshilfe Frauenheilkd. 2022 Dec 1;82(12):1337-1367. doi: 10.1055/a-1897-5124. eCollection 2022 Dec. Geburtshilfe Frauenheilkd. 2022. PMID: 36467974 Free PMC article.
-
Outcome and Management of Uterine Leiomyosarcoma Treated Following Surgery for Presumed Benign Disease: Review of Literature.Gynecol Minim Invasive Ther. 2018 Apr-Jun;7(2):47-55. doi: 10.4103/GMIT.GMIT_10_18. Epub 2018 May 2. Gynecol Minim Invasive Ther. 2018. PMID: 30254937 Free PMC article. Review.
-
Modern Myoma Treatment in the Last 20 Years: A Review of the Literature.Biomed Res Int. 2018 Jan 24;2018:4593875. doi: 10.1155/2018/4593875. eCollection 2018. Biomed Res Int. 2018. PMID: 29789793 Free PMC article. Review.
-
Correction: A Retrospective Analysis of the Impact of Myomectomy on Survival in Uterine Sarcoma.PLoS One. 2016 Apr 14;11(4):e0153996. doi: 10.1371/journal.pone.0153996. eCollection 2016. PLoS One. 2016. PMID: 27078148 Free PMC article. No abstract available.
References
-
- Olah KS, Dunn JA, Gee H. Leiomyosarcomas have a poorer prognosis than mixed mesodermal tumours when adjusting for known prognostic factors: the result of a retrospective study of 423 cases of uterine sarcoma. Br J Obstet Gynaecol 1992;99: 590–594. - PubMed
-
- Harlow BL, Weiss NS, Lofton S. The epidemiology of sarcomas of the uterus. J Natl Cancer Inst. 1986;76: 399–402. - PubMed
-
- Leibsohn S, d’Ablaing G, Mishell DR Jr, Schlaerth JB. Leiomyosarcoma in a series of hysterectomies performed for presumed uterineleiomyomas. Am J Obstet Gynecol. 1990;162: 968–976. - PubMed
-
- Parker WH, Fu YS, Berek JS. Uterine sarcoma in patients operated on for presumed leiomyoma and rapidly growing leiomyoma. Obstet Gynecol. 1994;83: 414–418. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
