

Genetic Variation in the Vesicular Monoamine Transporter: Preliminary Associations With Cognitive Outcomes After Severe Traumatic Brain Injury
- PMID: 26828714
- PMCID: PMC4967045
- DOI: 10.1097/HTR.0000000000000224
Genetic Variation in the Vesicular Monoamine Transporter: Preliminary Associations With Cognitive Outcomes After Severe Traumatic Brain Injury
Abstract
Introduction: Traumatic brain injury (TBI) frequently results in impaired cognition, a function that can be modulated by monoaminergic signaling. Genetic variation among monoaminergic genes may affect post-TBI cognitive performance. The vesicular monoamine transporter-2 (VMAT2) gene may be a novel source of genetic variation important for cognitive outcomes post-TBI given VMAT2's role in monoaminergic neurotransmission.
Objective: To evaluate associations between VMAT2 variability and cognitive outcomes post-TBI.
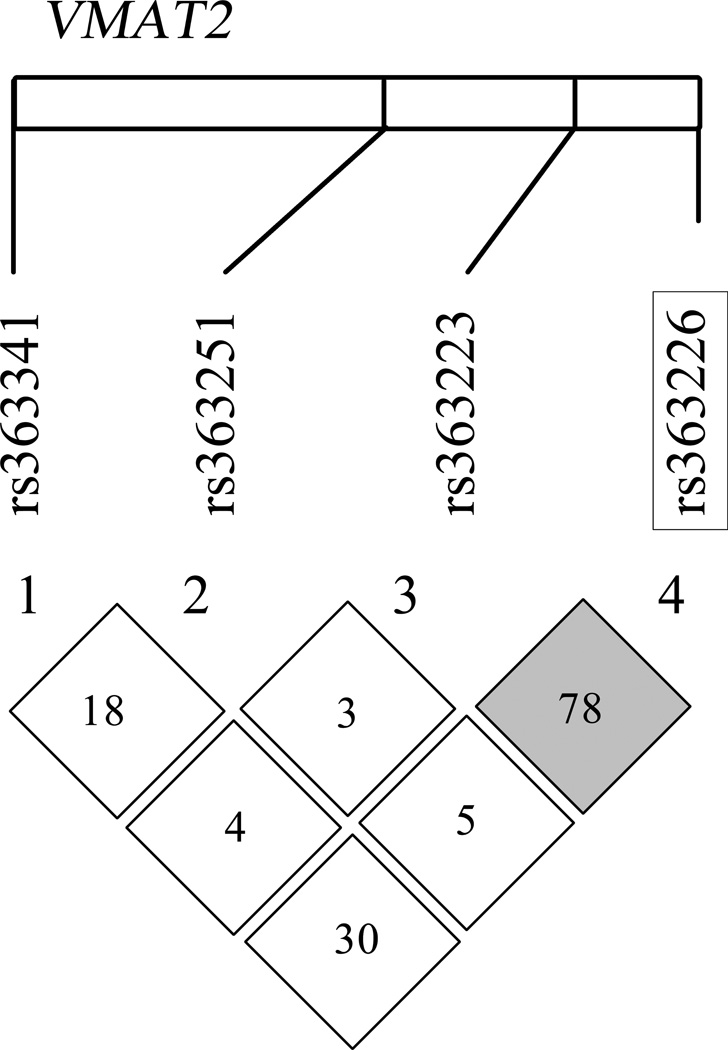
Methods: We evaluated 136 white adults with severe TBI for variation in VMAT2 using a tagging single nucleotide polymorphism (tSNP) approach (rs363223, rs363226, rs363251, and rs363341). We show genetic variation interacts with assessed cognitive impairment (cognitive composite [Comp-Cog] T-scores) to influence functional cognition (functional independence measure cognitive [FIM-Cog] subscale] 6 and 12 months postinjury.
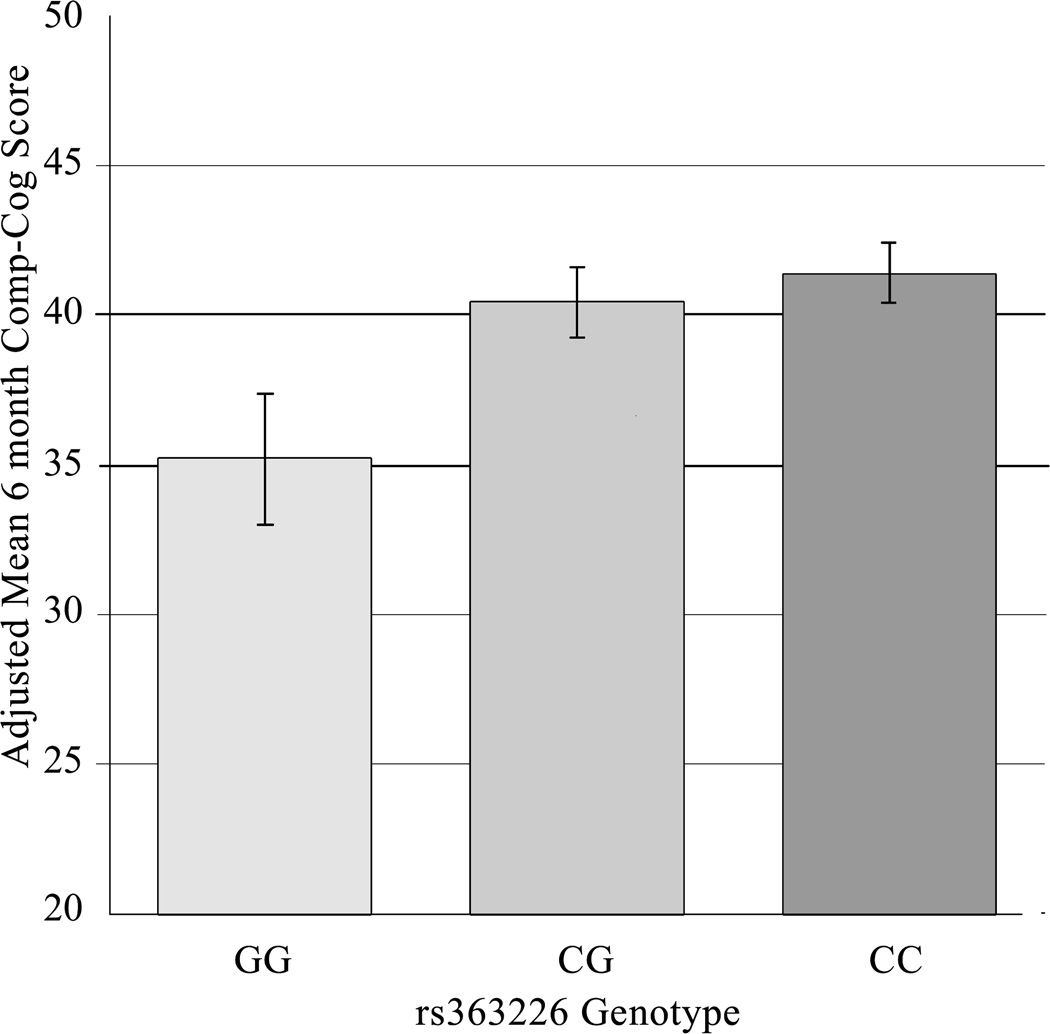
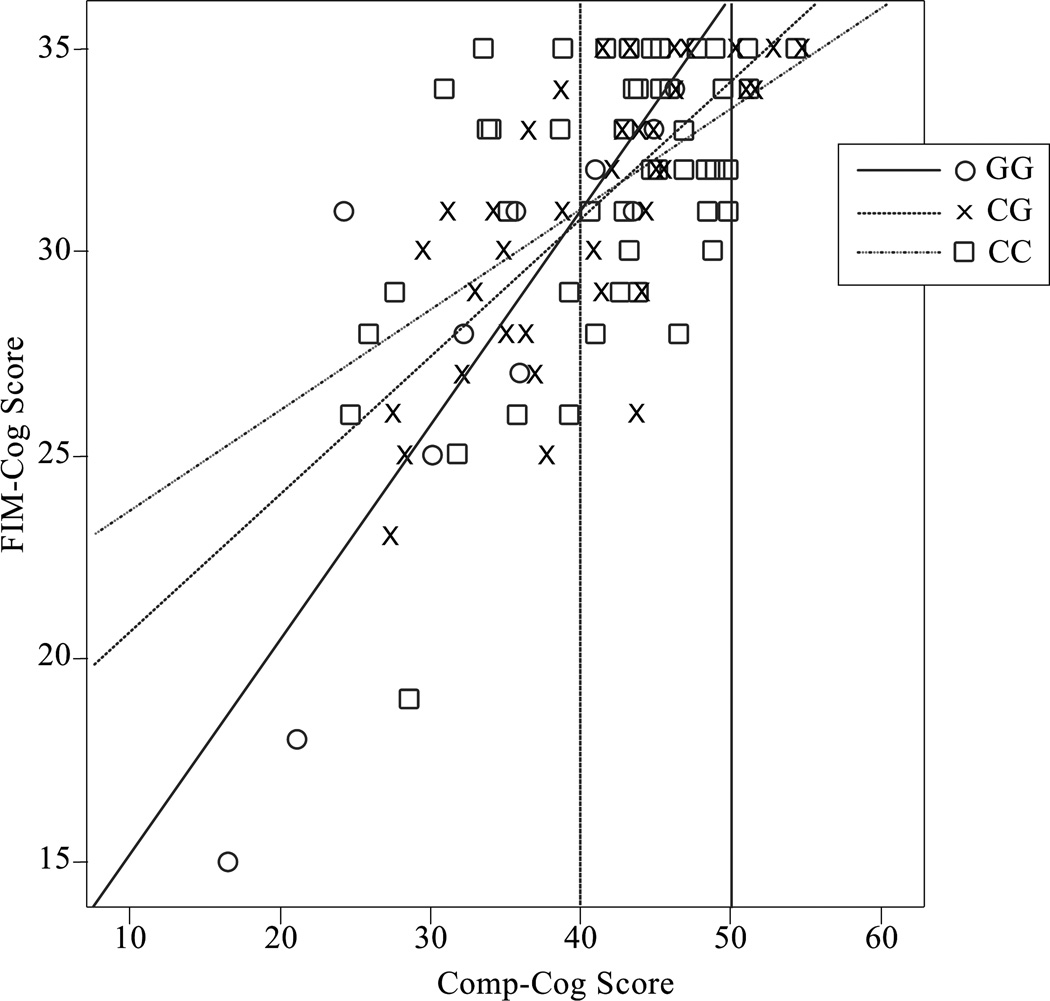
Results: Multivariate analyses at 6 months postinjury showed rs363226 genotype was associated with Comp-Cog (P = .040) and interacted with Comp-Cog to influence functional cognition (P < .001). G-homozygotes had the largest cognitive impairment, and their cognitive impairment had the greatest adverse effect on functional cognition.
Discussion: We provide the first evidence that genetic variation within VMAT2 is associated with cognitive outcomes after TBI. Further work is needed to validate this finding and elucidate mechanisms by which genetic variation affects monoaminergic signaling, mediating differences in cognitive outcomes.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Posttraumatic Brain Injury Cognitive Performance Is Moderated by Variation Within ANKK1 and DRD2 Genes.J Head Trauma Rehabil. 2015 Nov-Dec;30(6):E54-66. doi: 10.1097/HTR.0000000000000118. J Head Trauma Rehabil. 2015. PMID: 25931179 Free PMC article.
-
A Dopamine Pathway Gene Risk Score for Cognitive Recovery Following Traumatic Brain Injury: Methodological Considerations, Preliminary Findings, and Interactions With Sex.J Head Trauma Rehabil. 2016 Sep-Oct;31(5):E15-29. doi: 10.1097/HTR.0000000000000199. J Head Trauma Rehabil. 2016. PMID: 26580694
-
Preliminary Associations Between Brain-Derived Neurotrophic Factor, Memory Impairment, Functional Cognition, and Depressive Symptoms Following Severe TBI.Neurorehabil Neural Repair. 2016 Jun;30(5):419-30. doi: 10.1177/1545968315600525. Epub 2015 Aug 13. Neurorehabil Neural Repair. 2016. PMID: 26276123 Free PMC article.
-
Amantadine to Treat Cognitive Dysfunction in Moderate to Severe Traumatic Brain Injury.J Trauma Nurs. 2015 Jul-Aug;22(4):194-203; quiz E1-2. doi: 10.1097/JTN.0000000000000138. J Trauma Nurs. 2015. PMID: 26165872 Review.
-
Genetic drivers of cerebral blood flow dysfunction in TBI: a speculative synthesis.Nat Rev Neurol. 2019 Jan;15(1):25-39. doi: 10.1038/s41582-018-0105-9. Nat Rev Neurol. 2019. PMID: 30546123 Review.
Cited by
-
The pharmacogenomics of severe traumatic brain injury.Pharmacogenomics. 2017 Oct;18(15):1413-1425. doi: 10.2217/pgs-2017-0073. Epub 2017 Oct 4. Pharmacogenomics. 2017. PMID: 28975867 Free PMC article. Review.
-
Stretch Injury of Human Induced Pluripotent Stem Cell Derived Neurons in a 96 Well Format.Sci Rep. 2016 Sep 27;6:34097. doi: 10.1038/srep34097. Sci Rep. 2016. PMID: 27671211 Free PMC article.
-
Genetic Influences on Patient-Oriented Outcomes in Traumatic Brain Injury: A Living Systematic Review of Non-Apolipoprotein E Single-Nucleotide Polymorphisms.J Neurotrauma. 2021 Apr 15;38(8):1107-1123. doi: 10.1089/neu.2017.5583. Epub 2019 Jun 7. J Neurotrauma. 2021. PMID: 29799308 Free PMC article.
-
TBI Rehabilomics Research: an Exemplar of a Biomarker-Based Approach to Precision Care for Populations with Disability.Curr Neurol Neurosci Rep. 2017 Sep 19;17(11):84. doi: 10.1007/s11910-017-0791-5. Curr Neurol Neurosci Rep. 2017. PMID: 28929311 Review.
-
Toward a global and reproducible science for brain imaging in neurotrauma: the ENIGMA adult moderate/severe traumatic brain injury working group.Brain Imaging Behav. 2021 Apr;15(2):526-554. doi: 10.1007/s11682-020-00313-7. Brain Imaging Behav. 2021. PMID: 32797398 Free PMC article.
References
-
- Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21(5):375–378. - PubMed
-
- Cristofori I, Levin HS. Traumatic brain injury and cognition. Handb Clin Neurol. 2015;128:579–611. - PubMed
-
- Thurman DJ, et al. Traumatic brain injury in the United States: A public health perspective. J Head Trauma Rehabil. 1999;14(6):602–615. - PubMed
-
- Arciniegas DB, Held K, Wagner P. Cognitive Impairment Following Traumatic Brain Injury. Curr Treat Options Neurol. 2002;4(1):43–57. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
