

Combining Dopaminergic Facilitation with Robot-Assisted Upper Limb Therapy in Stroke Survivors: A Focused Review
- PMID: 26829074
- PMCID: PMC4866584
- DOI: 10.1097/PHM.0000000000000438
Combining Dopaminergic Facilitation with Robot-Assisted Upper Limb Therapy in Stroke Survivors: A Focused Review
Abstract
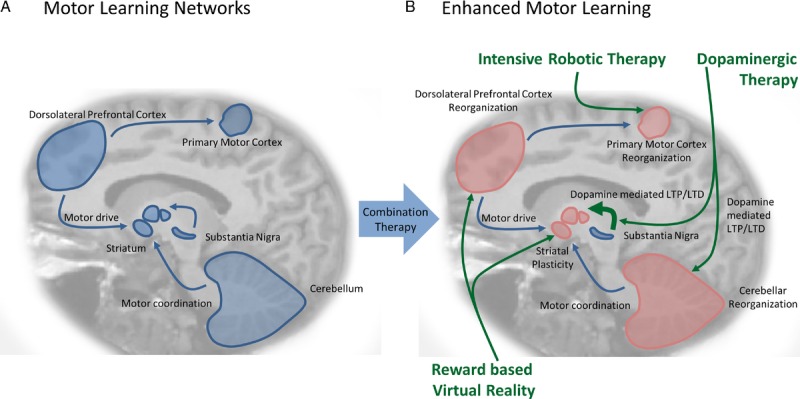
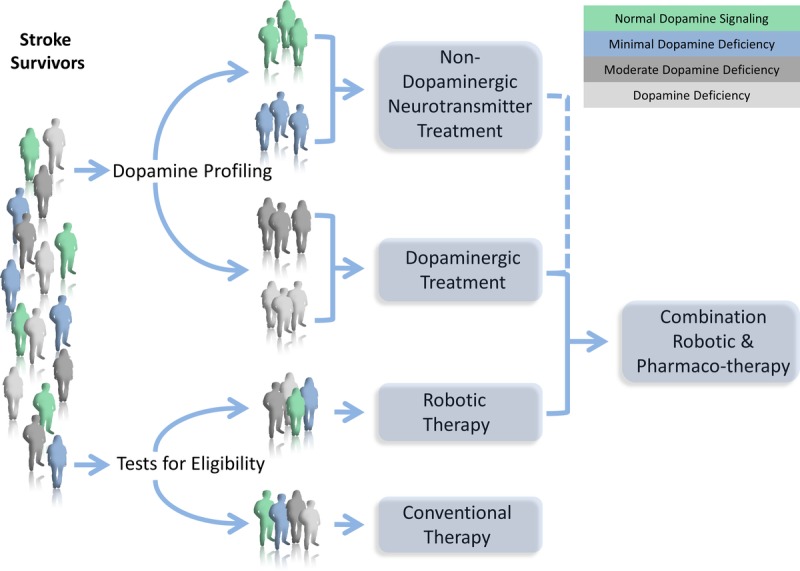
Despite aggressive conventional therapy, lasting hemiplegia persists in a large percentage of stroke survivors. The aim of this article is to critically review the rationale behind targeting multiple sites along the motor learning network by combining robotic therapy with pharmacotherapy and virtual reality-based reward learning to alleviate upper extremity impairment in stroke survivors. Methods for personalizing pharmacologic facilitation to each individual's unique biology are also reviewed. At the molecular level, treatment with levodopa was shown to induce long-term potentiation-like and practice-dependent plasticity. Clinically, trials combining conventional therapy with levodopa in stroke survivors yielded statistically significant but clinically unconvincing outcomes because of limited personalization, standardization, and reproducibility. Robotic therapy can induce neuroplasticity by delivering intensive, reproducible, and functionally meaningful interventions that are objective enough for the rigors of research. Robotic therapy also provides an apt platform for virtual reality, which boosts learning by engaging reward circuits. The future of stroke rehabilitation should target distinct molecular, synaptic, and cortical sites through personalized multimodal treatments to maximize motor recovery.
Figures
References
-
- Langhorne P, Coupar F, Pollock A: Motor recovery after stroke: A systematic review. Lancet Neurol 2009; 8: 741– 54 - PubMed
-
- Warlow CP, van Gijn J, Dennis MS, et al. Stroke: Practical Management. Malden, MA: Blackwell Publishing, 2008
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
