

Neuromuscular Effects of Common Krait (Bungarus caeruleus) Envenoming in Sri Lanka
- PMID: 26829229
- PMCID: PMC4734751
- DOI: 10.1371/journal.pntd.0004368
Neuromuscular Effects of Common Krait (Bungarus caeruleus) Envenoming in Sri Lanka
Abstract
Objective: We aimed to investigate neurophysiological and clinical effects of common krait envenoming, including the time course and treatment response.
Methodology: Patients with definite common krait (Bungarus caeruleus) bites were recruited from a Sri Lankan hospital. All patients had serial neurological examinations and stimulated concentric needle single-fibre electromyography (sfEMG) of orbicularis oculi in hospital at 6 wk and 6-9 mth post-bite.
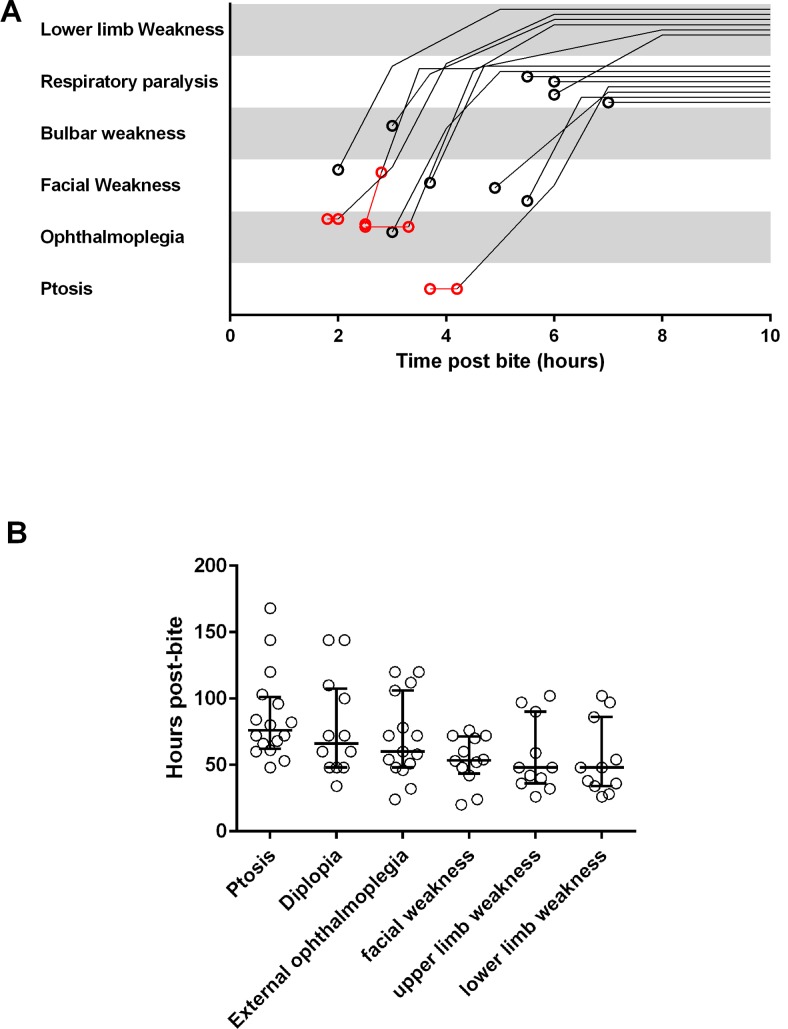
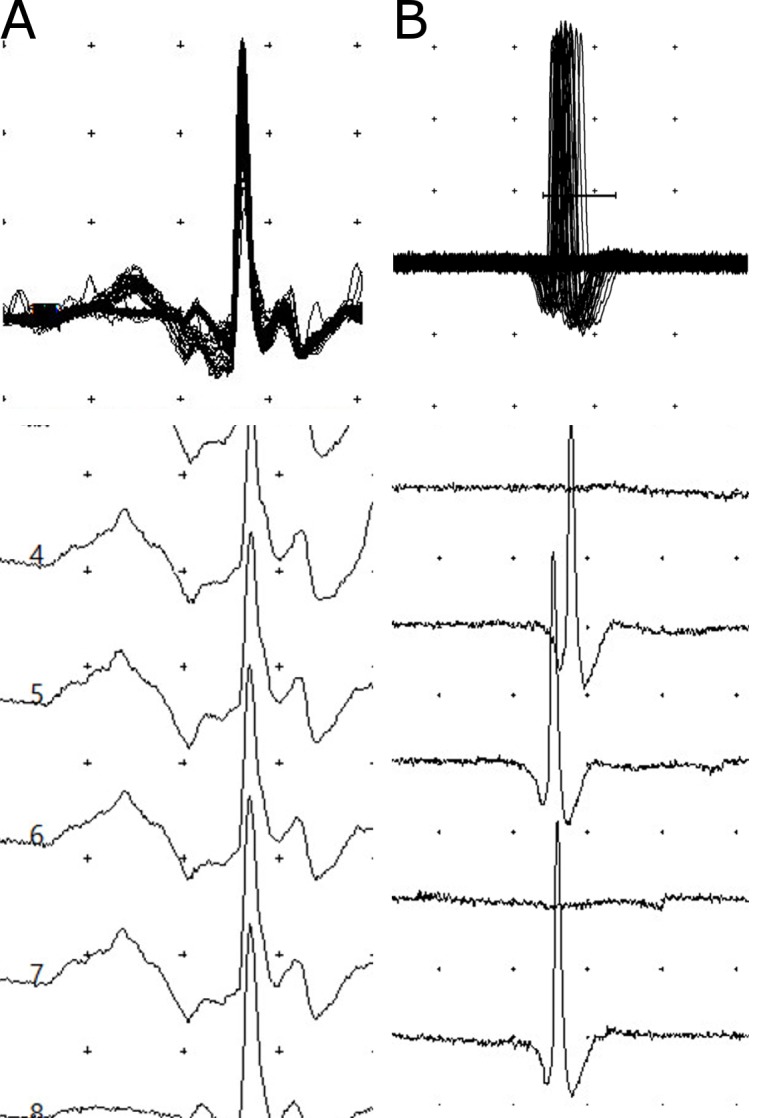
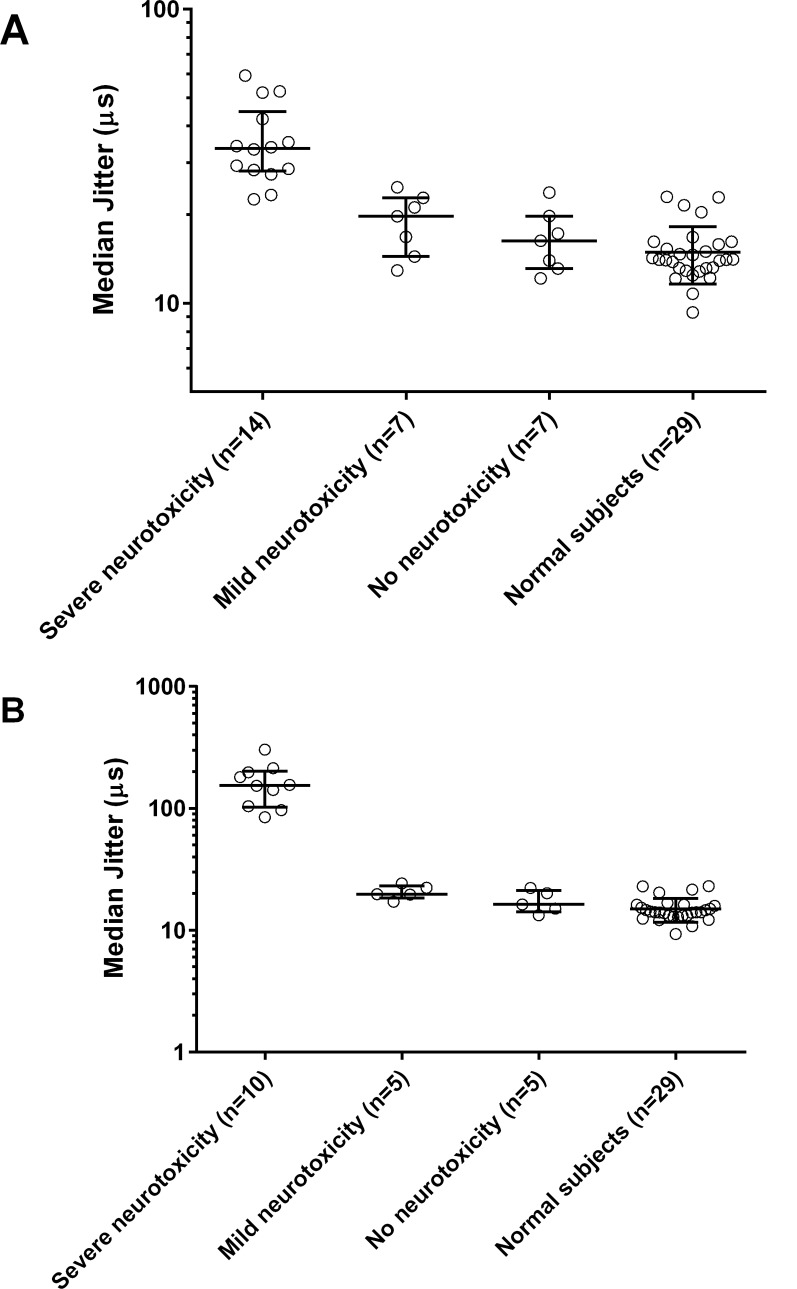
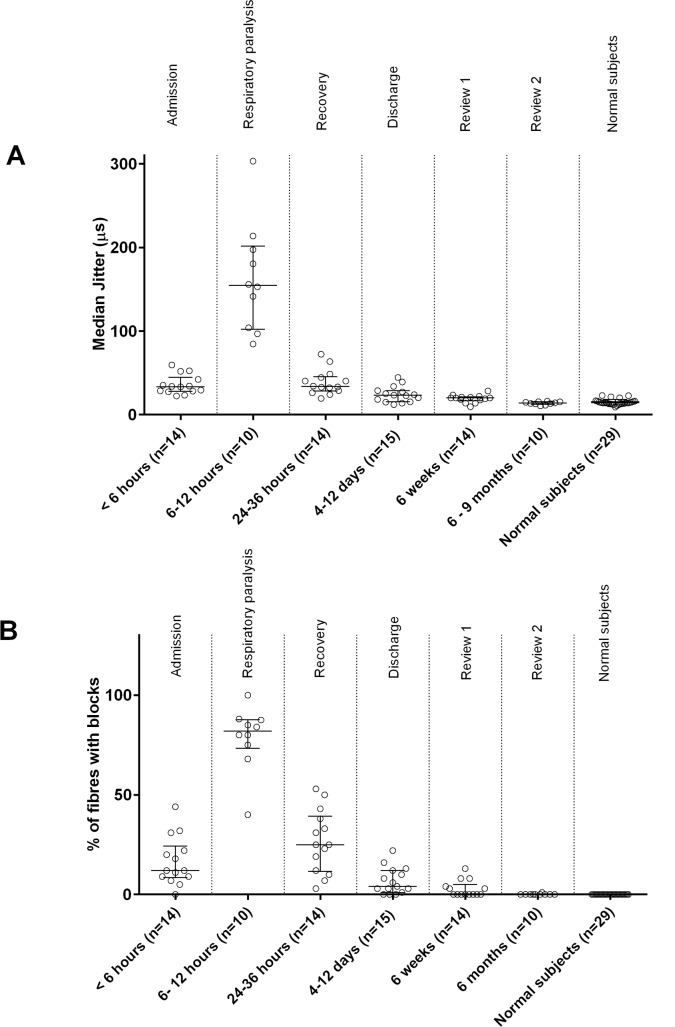
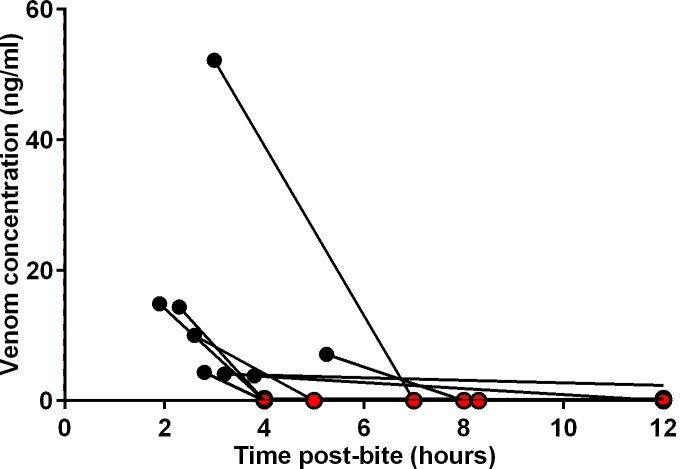
Principal findings: There were 33 patients enrolled (median age 35 y; 24 males). Eight did not develop neurotoxicity and had normal sfEMG. Eight had mild neurotoxicity with ptosis, normal sfEMG; six received antivenom and all recovered within 20-32 h. Seventeen patients developed severe neurotoxicity with rapidly descending paralysis, from ptosis to complete ophthalmoplegia, facial, bulbar and neck weakness. All 17 received Indian polyvalent antivenom a median 3.5 h post-bite (2.8-7.2 h), which cleared unbound venom from blood. Despite this, the paralysis worsened requiring intubation and ventilation within 7 h post-bite. sfEMG showed markedly increased jitter and neuromuscular blocks within 12 h. sfEMG abnormalities gradually improved over 24 h, corresponding with clinical recovery. Muscle recovery occurred in ascending order. Myotoxicity was not evident, clinically or biochemically, in any of the patients. Patients were extubated a median 96 h post-bite (54-216 h). On discharge, median 8 days (4-12 days) post-bite, patients were clinically normal but had mild sfEMG abnormalities which persisted at 6 wk post-bite. There were no clinical or neurophysiological abnormalities at 6-9 mth.
Conclusions: Common krait envenoming causes rapid onset severe neuromuscular paralysis which takes days to recover clinically consistent with sfEMG. Subclinical neuromuscular dysfunction lasts weeks but was not permanent. Antivenom effectively cleared venom but did not prevent worsening or reverse neuromuscular paralysis.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Neurotoxicity in Russell's viper (Daboia russelii) envenoming in Sri Lanka: a clinical and neurophysiological study.Clin Toxicol (Phila). 2016 Jun;54(5):411-9. doi: 10.3109/15563650.2016.1143556. Epub 2016 Feb 29. Clin Toxicol (Phila). 2016. PMID: 26923566
-
Confirmed Ceylon krait (Bungarus ceylonicus) envenoming in Sri Lanka resulting in neuromuscular paralysis: a case report.J Med Case Rep. 2017 Nov 24;11(1):330. doi: 10.1186/s13256-017-1503-0. J Med Case Rep. 2017. PMID: 29169382 Free PMC article.
-
Venomics of Bungarus caeruleus (Indian krait): Comparable venom profiles, variable immunoreactivities among specimens from Sri Lanka, India and Pakistan.J Proteomics. 2017 Jul 5;164:1-18. doi: 10.1016/j.jprot.2017.04.018. Epub 2017 May 2. J Proteomics. 2017. PMID: 28476572
-
Antivenom for Neuromuscular Paralysis Resulting From Snake Envenoming.Toxins (Basel). 2017 Apr 19;9(4):143. doi: 10.3390/toxins9040143. Toxins (Basel). 2017. PMID: 28422078 Free PMC article. Review.
-
Kraits of Indian subcontinent: Natural history, risks, venom variation, lethality and treatment strategies - A comprehensive review.Toxicon. 2025 Jul;262:108406. doi: 10.1016/j.toxicon.2025.108406. Epub 2025 May 13. Toxicon. 2025. PMID: 40374096 Review.
Cited by
-
Engineered nanoparticles bind elapid snake venom toxins and inhibit venom-induced dermonecrosis.PLoS Negl Trop Dis. 2018 Oct 4;12(10):e0006736. doi: 10.1371/journal.pntd.0006736. eCollection 2018 Oct. PLoS Negl Trop Dis. 2018. PMID: 30286075 Free PMC article.
-
Neuromuscular Weakness and Paralysis Produced by Snakebite Envenoming: Mechanisms and Proposed Standards for Clinical Assessment.Toxins (Basel). 2023 Jan 6;15(1):49. doi: 10.3390/toxins15010049. Toxins (Basel). 2023. PMID: 36668869 Free PMC article. Review.
-
A Pharmacological Examination of the Cardiovascular Effects of Malayan Krait (Bungarus candidus) Venoms.Toxins (Basel). 2017 Mar 29;9(4):122. doi: 10.3390/toxins9040122. Toxins (Basel). 2017. PMID: 28353659 Free PMC article.
-
Development of a Treatment Protocol for Cobra (Naja naja) Bite Envenoming in Dogs.Toxins (Basel). 2020 Nov 2;12(11):694. doi: 10.3390/toxins12110694. Toxins (Basel). 2020. PMID: 33147770 Free PMC article.
-
A Nationwide Study on the Risks of Complications and Healthcare Costs of Snakebite Envenomation in Taiwan.Am J Trop Med Hyg. 2024 May 7;111(1):205-215. doi: 10.4269/ajtmh.24-0030. Print 2024 Jul 3. Am J Trop Med Hyg. 2024. PMID: 38714189 Free PMC article.
References
-
- Isbister GK, Brown SG, Page CB, McCoubrie DL, Greene SL, Buckley N a. Snakebite in Australia: A practical approach to diagnosis and treatment. Med J Aust. 2013;199: 763–768. - PubMed
-
- Valenta J. Venmous snakes—Envenoming, Therapy 2nd Edition New York: Nova Science Publishers, Inc.; 2010.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
