

Comparison of Insulin Resistance to Coronary Atherosclerosis in Human Immunodeficiency Virus Infected and Uninfected Men (from the Multicenter AIDS Cohort Study)
- PMID: 26830260
- PMCID: PMC4775332
- DOI: 10.1016/j.amjcard.2015.12.037
Comparison of Insulin Resistance to Coronary Atherosclerosis in Human Immunodeficiency Virus Infected and Uninfected Men (from the Multicenter AIDS Cohort Study)
Abstract
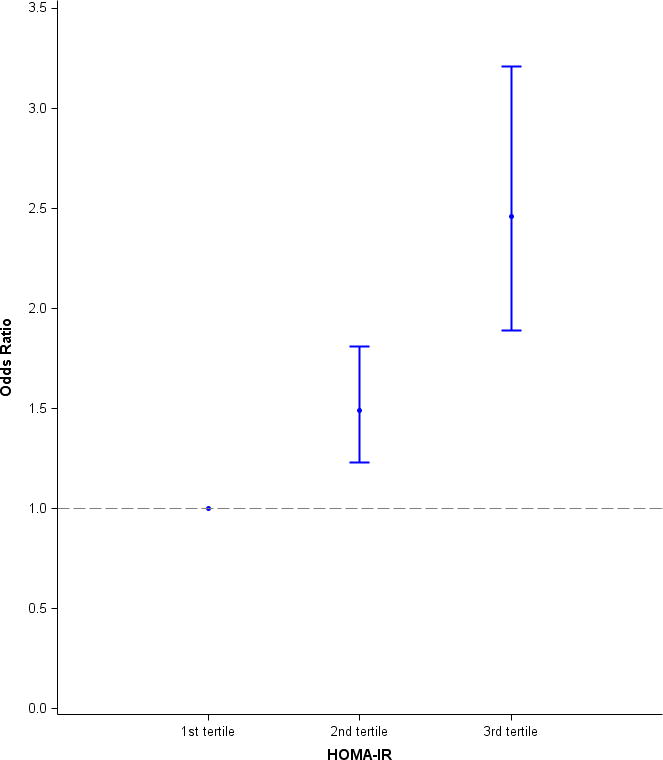
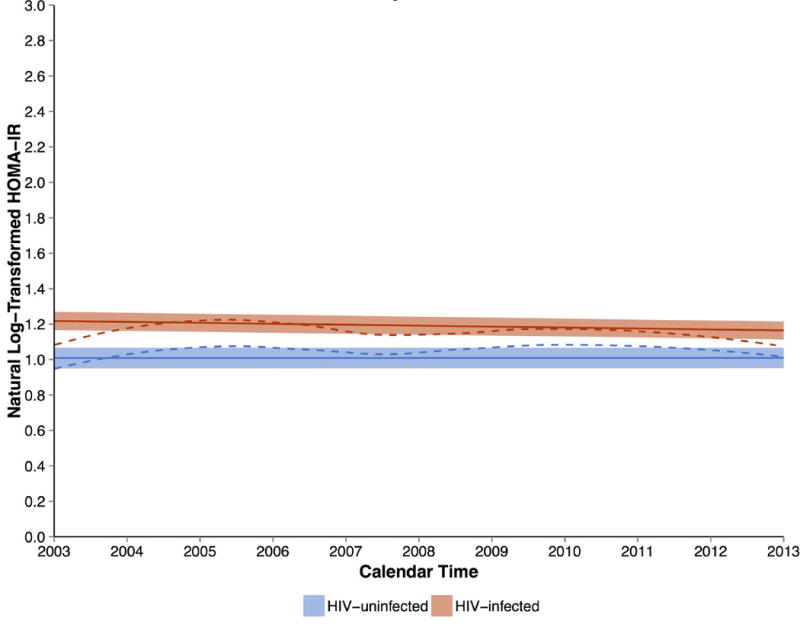
The relation between insulin resistance (IR) and coronary artery disease in patients with human immunodeficiency virus (HIV) infection remains incompletely defined. Fasting serum insulin and glucose measurements from 448 HIV-infected and 306 uninfected men enrolled in the Multicenter AIDS Cohort Study were collected at semiannual visits from 2003 to 2013 and used to compute the homeostatic model assessment of IR (HOMA-IR). Coronary computed tomographic angiography (CTA) was performed at the end of the study period to characterize coronary pathology. Associations between HOMA-IR (categorized into tertiles and assessed near the time of the CTA and over the 10-year study period) and the prevalence of coronary plaque or stenosis ≥50% were assessed with multivariate logistic regression. HOMA-IR was higher in HIV-infected men than HIV-uninfected men when measured near the time of CTA (3.2 vs 2.7, p = 0.002) and when averaged over the study period (3.4 vs 3.0, p <0.001). The prevalence of coronary stenosis ≥50% was similar between both groups (17% vs 15%, p = 0.41). Both measurements of HOMA-IR were associated with greater odds of coronary stenosis ≥50% in models comparing men with values in the highest versus the lowest tertiles, although the effect of mean HOMA-IR was stronger than the single measurement of HOMA-IR before CTA (odds ratio 2.46, 95% CI 1.95 to 3.11, vs odds ratio 1.43, 1.20 to 1.70). This effect was not significantly modified by HIV serostatus. In conclusion, IR over nearly a decade was greater in HIV-infected men than HIV-uninfected men, and in both groups, was associated with significant coronary artery stenosis.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Low thigh muscle mass is associated with coronary artery stenosis among HIV-infected and HIV-uninfected men: The Multicenter AIDS Cohort Study (MACS).J Cardiovasc Comput Tomogr. 2018 Mar-Apr;12(2):131-138. doi: 10.1016/j.jcct.2018.01.007. Epub 2018 Jan 31. J Cardiovasc Comput Tomogr. 2018. PMID: 29396194 Free PMC article.
-
Insulin resistance is associated with coronary plaque vulnerability: insight from optical coherence tomography analysis.Eur Heart J Cardiovasc Imaging. 2014 Mar;15(3):284-91. doi: 10.1093/ehjci/jet158. Epub 2013 Sep 9. Eur Heart J Cardiovasc Imaging. 2014. PMID: 24022065
-
Insulin resistance is associated with significant clinical atherosclerosis in nondiabetic patients with acute myocardial infarction.Arterioscler Thromb Vasc Biol. 2013 Sep;33(9):2245-51. doi: 10.1161/ATVBAHA.113.301585. Epub 2013 Jul 18. Arterioscler Thromb Vasc Biol. 2013. PMID: 23868937 Free PMC article.
-
Association of HIV Infection With Cardiovascular Pathology Based on Advanced Cardiovascular Imaging: A Systematic Review.JAMA. 2022 Sep 13;328(10):951-962. doi: 10.1001/jama.2022.15078. JAMA. 2022. PMID: 36098725 Free PMC article.
-
Association between the homeostasis model assessment of insulin resistance and coronary artery calcification: a meta-analysis of observational studies.Front Endocrinol (Lausanne). 2023 Nov 27;14:1271857. doi: 10.3389/fendo.2023.1271857. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 38089605 Free PMC article.
Cited by
-
Cardiac Steatosis in HIV-A Marker or Mediator of Disease?Front Endocrinol (Lausanne). 2018 Oct 11;9:529. doi: 10.3389/fendo.2018.00529. eCollection 2018. Front Endocrinol (Lausanne). 2018. PMID: 30364255 Free PMC article. Review.
-
Metabolic health across the BMI spectrum in HIV-infected and HIV-uninfected men.AIDS. 2018 Jan 2;32(1):49-57. doi: 10.1097/QAD.0000000000001651. AIDS. 2018. PMID: 28926404 Free PMC article.
-
Factors Associated With Insulin Resistance in Adults With HIV Receiving Contemporary Antiretroviral Therapy: a Brief Update.Curr HIV/AIDS Rep. 2018 Jun;15(3):223-232. doi: 10.1007/s11904-018-0399-7. Curr HIV/AIDS Rep. 2018. PMID: 29700760 Free PMC article. Review.
-
Metabolic Complications and Glucose Metabolism in HIV Infection: A Review of the Evidence.Curr HIV/AIDS Rep. 2016 Oct;13(5):289-96. doi: 10.1007/s11904-016-0330-z. Curr HIV/AIDS Rep. 2016. PMID: 27541600 Free PMC article. Review.
-
CX3CL1-Fc treatment prevents atherosclerosis in Ldlr KO mice.Mol Metab. 2019 Feb;20:89-101. doi: 10.1016/j.molmet.2018.11.011. Epub 2018 Dec 2. Mol Metab. 2019. PMID: 30553772 Free PMC article.
References
-
- Laakso M, Kuusisto J. Insulin resistance and hyperglycaemia in cardiovascular disease development. Nat Rev Endocrinol. 2014;10:293–302. - PubMed
-
- American College of Cardiology Foundation Task Force on Expert Consensus D. Mark DB, Berman DS, Budoff MJ, Carr JJ, Gerber TC, Hecht HS, Hlatky MA, Hodgson JM, Lauer MS, Miller JM, Morin RL, Mukherjee D, Poon M, Rubin GD, Schwartz RS. ACCF/ACR/AHA/NASCI/SAIP/SCAI/SCCT 2010 expert consensus document on coronary computed tomographic angiography: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. Circulation. 2010;121:2509–2543. - PubMed
-
- Guaraldi G, Zona S, Orlando G, Carli F, Ligabue G, Fiocchi F, Rossi R, Modena MG, Raggi P. Progression of coronary artery calcium in men affected by human immunodeficiency virus infection. Int J Cardiovasc Imaging. 2012;28:935–941. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 AI035042/AI/NIAID NIH HHS/United States
- UL1TR000124/TR/NCATS NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- K24AI120834/AI/NIAID NIH HHS/United States
- U01 AI35040/AI/NIAID NIH HHS/United States
- K24 AI120834/AI/NIAID NIH HHS/United States
- UL1 TR000124/TR/NCATS NIH HHS/United States
- U01-AI35042/AI/NIAID NIH HHS/United States
- U01 AI035041/AI/NIAID NIH HHS/United States
- UM1 AI035043/AI/NIAID NIH HHS/United States
- R01 HL095129/HL/NHLBI NIH HHS/United States
- U01-AI35041/AI/NIAID NIH HHS/United States
- U01 AI035043/AI/NIAID NIH HHS/United States
- U01-AI35039/AI/NIAID NIH HHS/United States
- U01 AI035040/AI/NIAID NIH HHS/United States
- U01 AI035039/AI/NIAID NIH HHS/United States
- UM1-AI35043/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
