

Stem cells of the suture mesenchyme in craniofacial bone development, repair and regeneration
- PMID: 26830436
- PMCID: PMC4740445
- DOI: 10.1038/ncomms10526
Stem cells of the suture mesenchyme in craniofacial bone development, repair and regeneration
Abstract
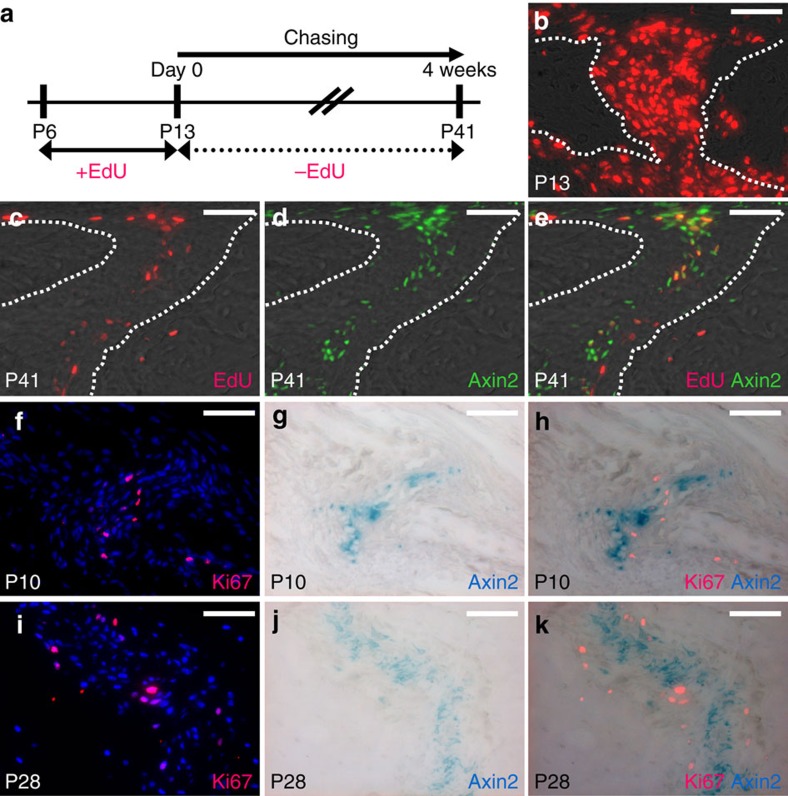
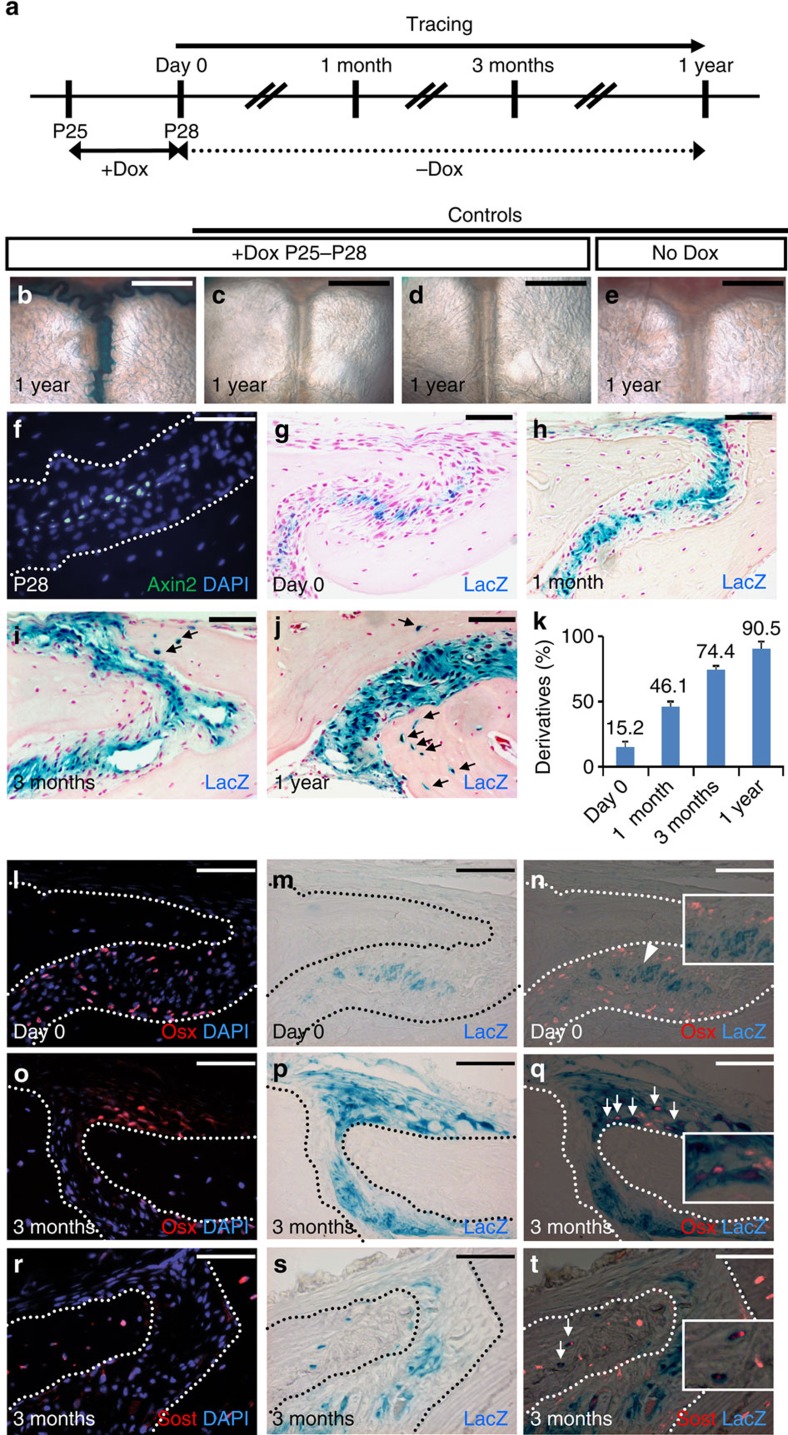
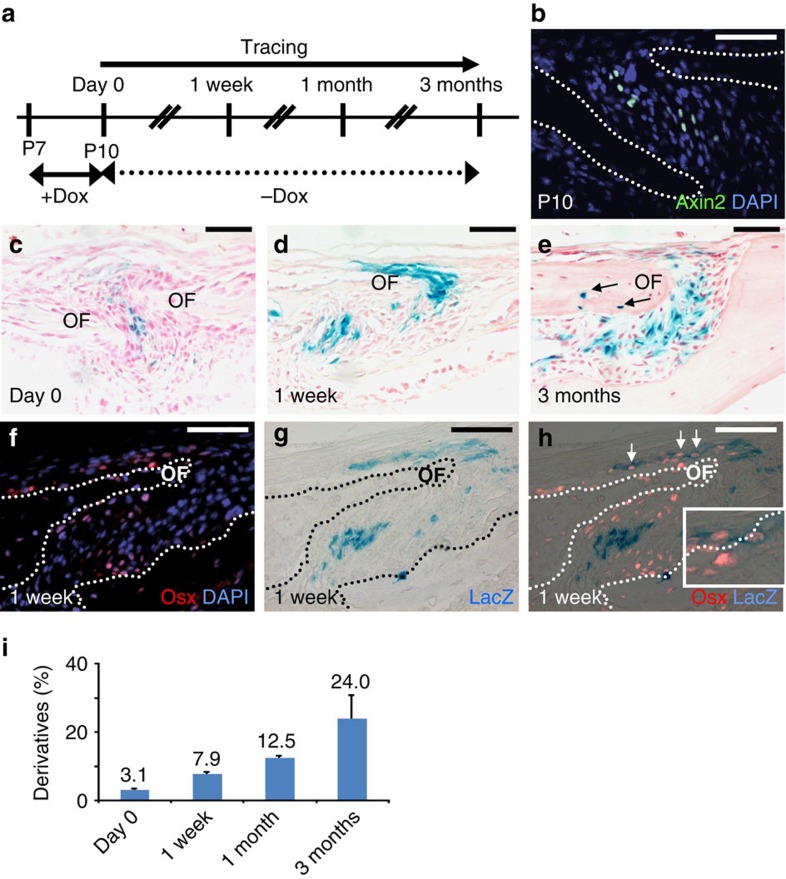
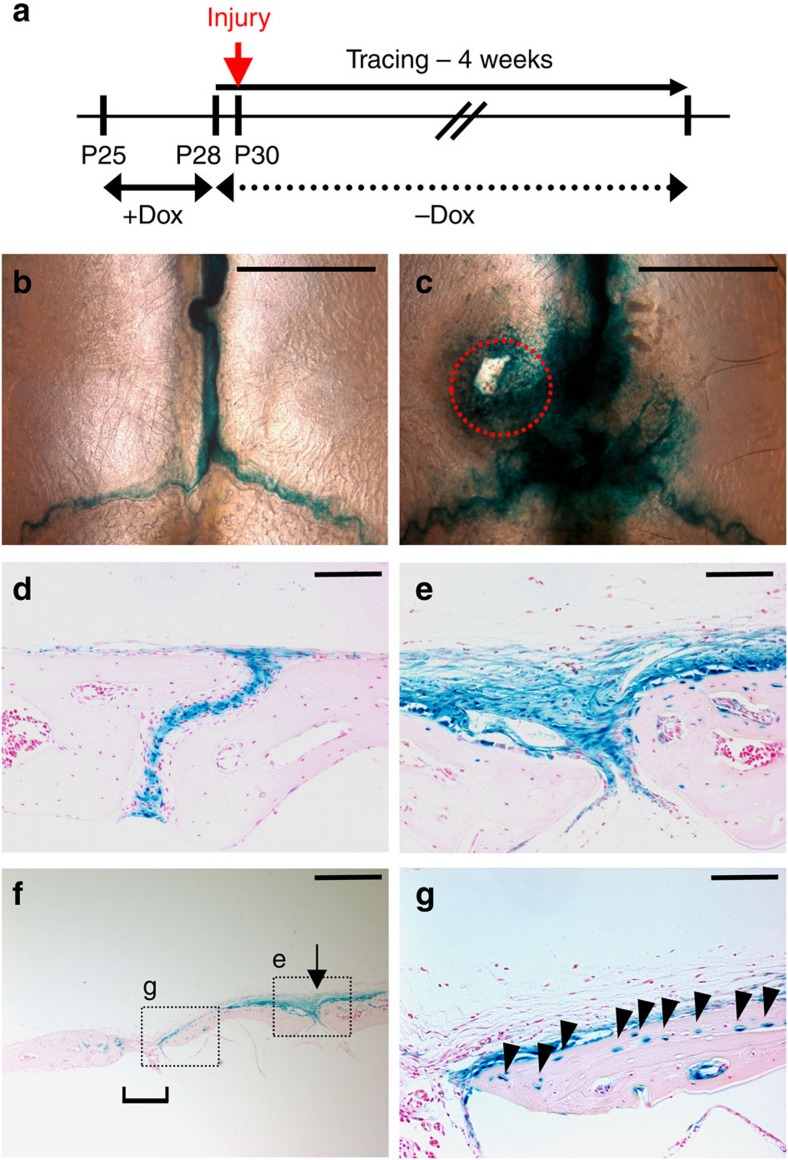
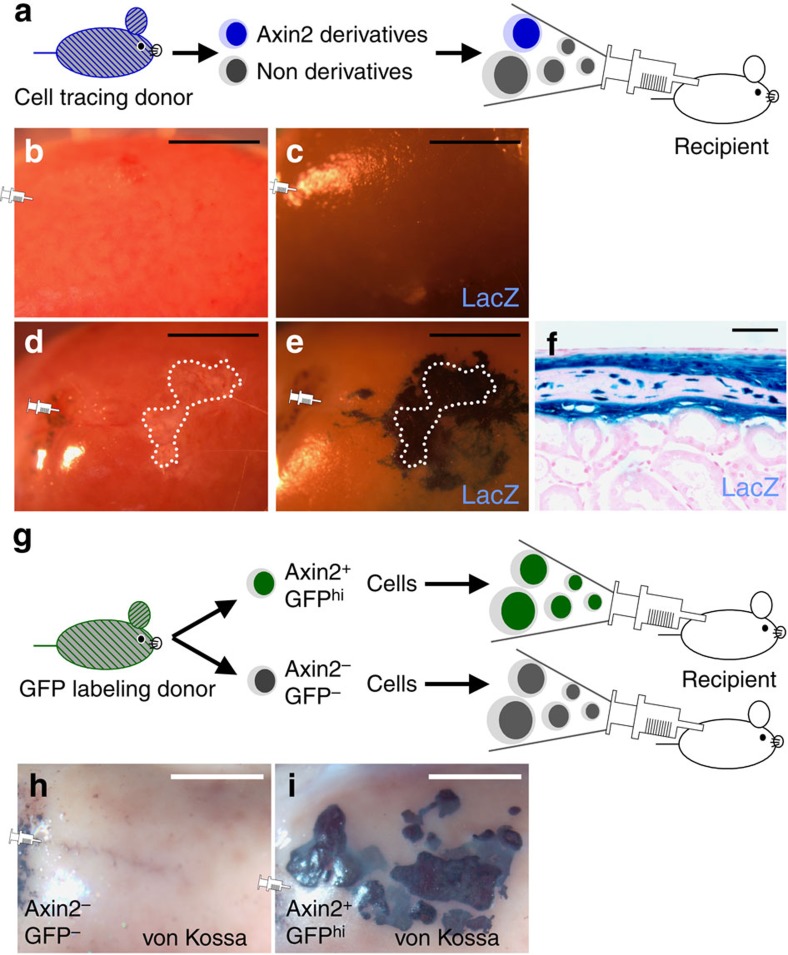
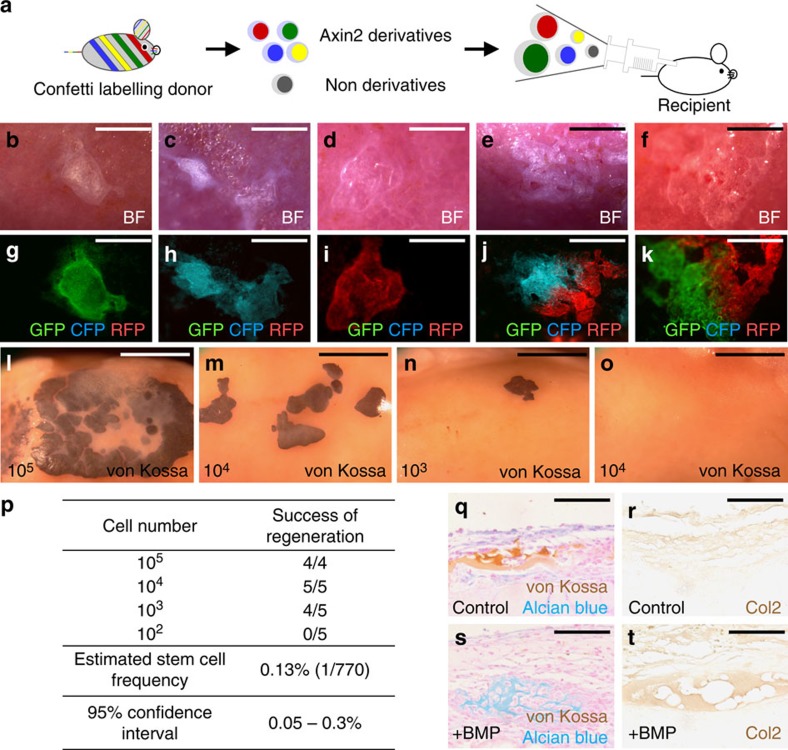
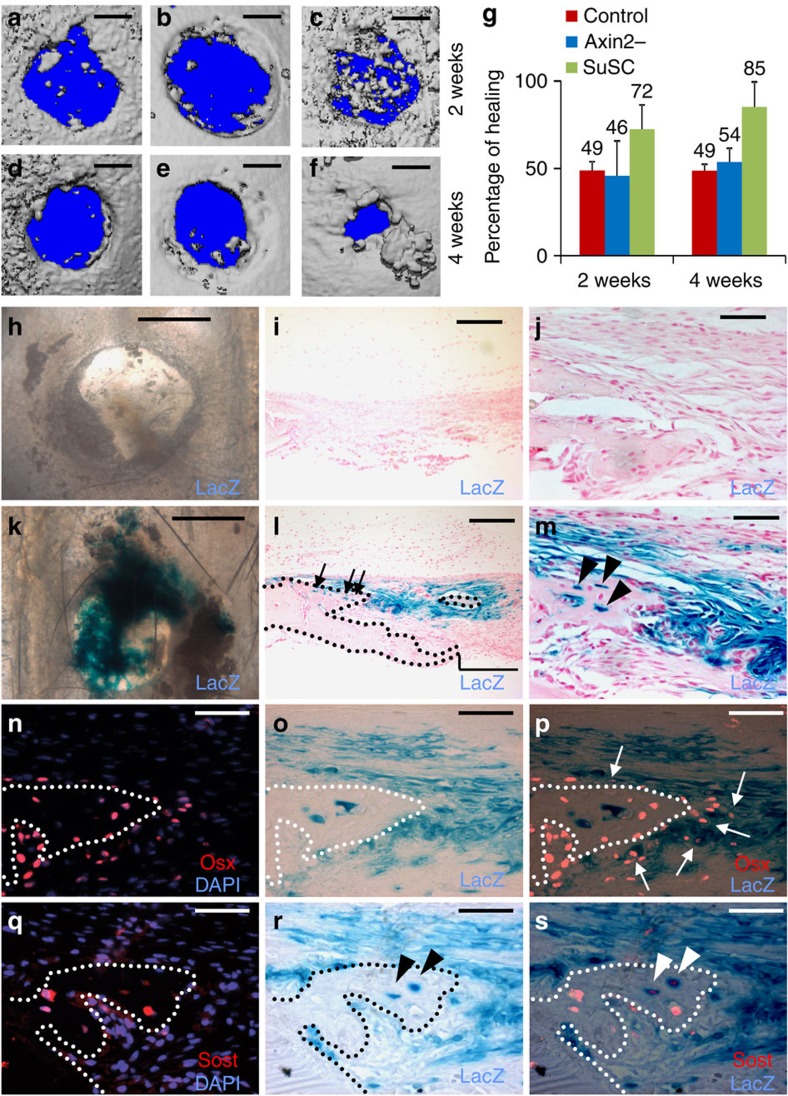
The suture mesenchyme serves as a growth centre for calvarial morphogenesis and has been postulated to act as the niche for skeletal stem cells. Aberrant gene regulation causes suture dysmorphogenesis resulting in craniosynostosis, one of the most common craniofacial deformities. Owing to various limitations, especially the lack of suture stem cell isolation, reconstruction of large craniofacial bone defects remains highly challenging. Here we provide the first evidence for an Axin2-expressing stem cell population with long-term self-renewing, clonal expanding and differentiating abilities during calvarial development and homeostastic maintenance. These cells, which reside in the suture midline, contribute directly to injury repair and skeletal regeneration in a cell autonomous fashion. Our findings demonstrate their true identity as skeletal stem cells with innate capacities to replace the damaged skeleton in cell-based therapy, and permit further elucidation of the stem cell-mediated craniofacial skeletogenesis, leading to revealing the complex nature of congenital disease and regenerative medicine.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
