

Inhalative steroids as an individual treatment in symptomatic lung cancer patients with radiation pneumonitis grade II after radiotherapy - a single-centre experience
- PMID: 26830686
- PMCID: PMC4736495
- DOI: 10.1186/s13014-016-0580-3
Inhalative steroids as an individual treatment in symptomatic lung cancer patients with radiation pneumonitis grade II after radiotherapy - a single-centre experience
Abstract
Purpose: To assess efficacy of our single-centre experience with inhalative steroids (IS) in lung cancer patients with symptomatic radiation pneumonitis (RP) grade II.
Material and methods: Between 05/09 and 07/10, 24 patients (female, n = 8; male, n = 16) with lung cancer (non-small cell lung carcinoma [NSCLC]: n = 19; small cell lung cancer [SCLC]: n = 3; unknown histology: n = 2) and good performance status (ECOG ≤1) received definitive radiotherapy to the primary tumour site and involved lymph nodes with concurrent chemotherapy (n = 18), sequential chemotherapy (n = 2) or radiation only (n = 4) and developed symptomatic RP grade II during follow-up. No patient presented with oxygen requiring RP grade III. The mean age at diagnosis was 66 years (range: 50-82 years). Nine patients suffered from chronic obstructive pulmonary disease (COPD) before treatment, and 18 patients had a smoking history (median pack years: 48). The mean lung dose was 15.5 Gy (range: 3.0-23.1 Gy). All patients were treated with IS. If a patient's clinical symptoms did not significantly improve within two weeks of IS therapy initiation, their treatment was switched to oral prednisolone.
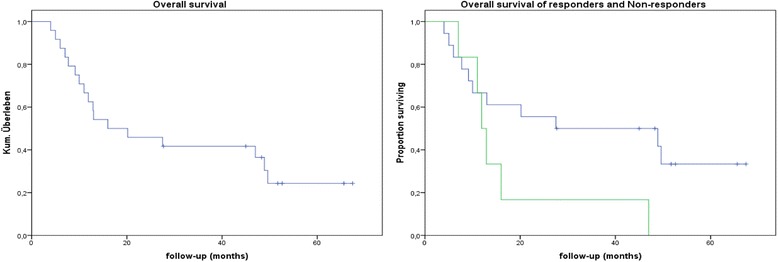
Results: All 24 patients were initially treated with a high dose IS (budesonide 800 μg 1-0-1) for 14 days. Of the patients, 18 showed a significant improvement of clinical symptoms and 6 patients did not show significant improvement of clinical symptoms and were classified as non-responders to IS. Their treatment was switched to oral steroids after two weeks (starting with oral prednisolone, 0.5 mg/kg bodyweight; at least 50 mg per day). All of these patients responded to the prednisolone. None of non-responders presented with increased symptoms of RP and required oxygen and / or hospitalization (RP grade III). The median follow-up after IS treatment initiation was 18 months (range: 4-66 months). The median duration of IS treatment and prednisolone treatment was 8.2 months (range: 3.0-48.3 months) and 11.4 months (range: 5.0-44.0 months), respectively. Of the 18 IS treatment responders, 2 (11.1 %) patients with pre-existing grade 2 COPD still required IS (400 μg twice a day) 45.0 and 48.3 months after radiotherapy, respectively. For the remaining 16 responders (88.9 %), IS therapy was stopped after 7.7 months (range: 3.0-18.2 months). None of the patients treated with IS developed any specific IS-related side effects such as oral candidiasis.
Conclusion: This single-centre experience shows that high-dose IS is an individual treatment option for radiation-induced pneumonitis grade II in patients with a good performance status.
Figures
References
-
- Christodoulou M, Bayman N, McCloskey P,Rowbottom C, Faivre-Finn C. New radiotherapy approaches in locally advanced non-small cell lung cancer. Eur J Cancer. 2014;50(3):525–34. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
