

Mechanical versus manual chest compressions for cardiac arrest: a systematic review and meta-analysis
- PMID: 26830837
- PMCID: PMC4736253
- DOI: 10.1186/s13049-016-0202-y
Mechanical versus manual chest compressions for cardiac arrest: a systematic review and meta-analysis
Abstract
Background: The aim of this paper was to conduct a systematic review of the published literatures comparing the use of mechanical chest compression device and manual chest compression during cardiac arrest (CA) with respect to short-term survival outcomes and neurological function.
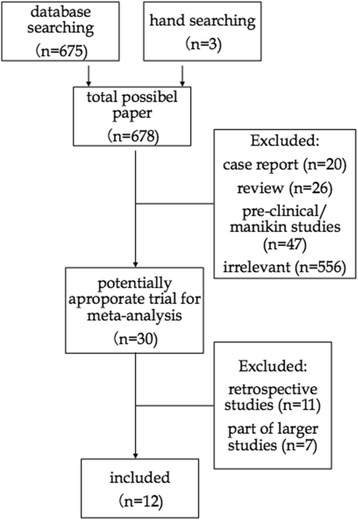
Methods: Databases including MEDLINE, EMBASE, Web of Science and the ClinicalTrials.gov registry were systematically searched. Further references were gathered from cross-references from articles by handsearch. The inclusion criteria for this review must be human prospective controlled studies of adult CA. Random effects models were used to assess the risk ratios and 95% confidence intervals for return of spontaneous circulation (ROSC), survival to admission and discharge, and neurological function.
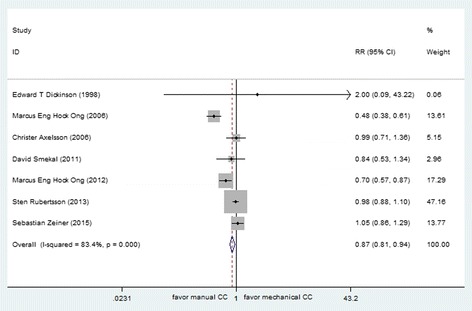
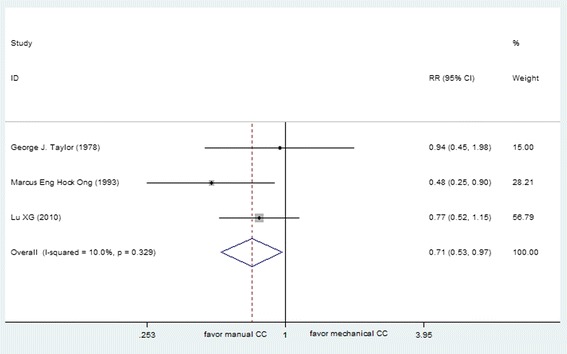
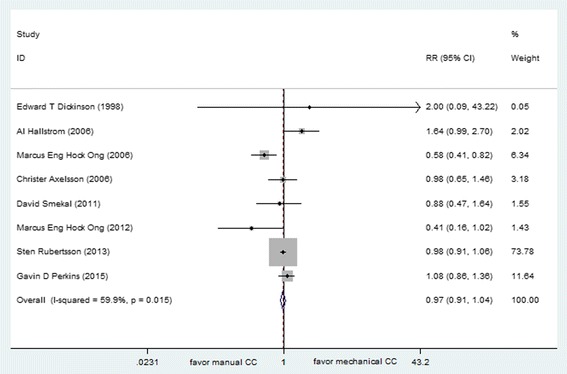
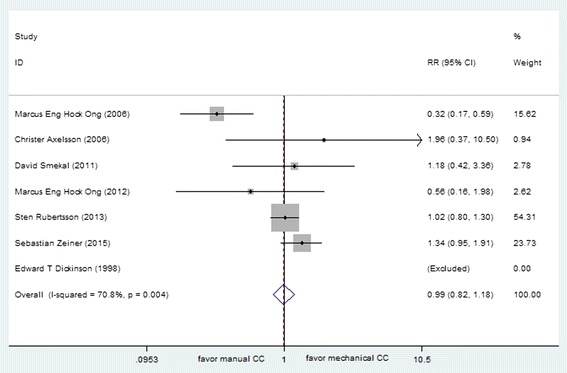
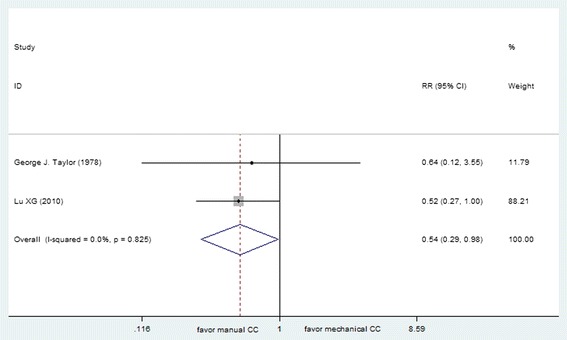
Results: Twelve trials (9 out-of-hospital and 3 in-hospital studies), involving 11,162 participants, were included in the review. The results of this meta-analysis indicated no differences were found in Cerebral Performance Category (CPC) scores, survival to hospital admission and survival to discharge between manual cardiopulmonary resuscitation (CPR) and mechanical CPR for out-of-hospital CA (OHCA) patients. The data on achieving ROSC in both of in-hospital and out-of-hospital setting suggested poor application of the mechanical device (RR 0.71, [95% CI, 0.53, 0.97] and 0.87 [95% CI, 0.81, 0.94], respectively). OHCA patients receiving manual resuscitation were more likely to attain ROSC compared with load-distributing bands chest compression device (RR 0.88, [95% CI, 0.80, 0.96]). The in-hospital studies suggested increased relative harm with mechanical compressions for ratio of survival to hospital discharge (RR 0.54, [95% CI 0.29, 0.98]). However, the results were not statistically significant between different kinds of mechanical chest compression devices and manual resuscitation in survival to admission, discharge and CPC scores for OHCA patients and survival to discharge for in-hospital CA patients.
Conclusions: The ability to achieve ROSC with mechanical devise was inferior to manual chest compression during resuscitation. The use of mechanical chest compression cannot be recommended as a replacement for manual CPR, but rather a supplemental treatment in an overall strategy for treating CA patients.
Figures


Similar articles
-
Continuous chest compression versus interrupted chest compression for cardiopulmonary resuscitation of non-asphyxial out-of-hospital cardiac arrest.Cochrane Database Syst Rev. 2017 Mar 27;3(3):CD010134. doi: 10.1002/14651858.CD010134.pub2. Cochrane Database Syst Rev. 2017. PMID: 28349529 Free PMC article.
-
Mechanical versus manual chest compressions for cardiac arrest.Cochrane Database Syst Rev. 2014 Feb 27;(2):CD007260. doi: 10.1002/14651858.CD007260.pub3. Cochrane Database Syst Rev. 2014. Update in: Cochrane Database Syst Rev. 2018 Aug 20;8:CD007260. doi: 10.1002/14651858.CD007260.pub4. PMID: 24574099 Updated.
-
Mechanical versus manual chest compressions for cardiac arrest.Cochrane Database Syst Rev. 2011 Jan 19;(1):CD007260. doi: 10.1002/14651858.CD007260.pub2. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2014 Feb 27;(2):CD007260. doi: 10.1002/14651858.CD007260.pub3. PMID: 21249689 Updated.
-
Effectiveness of Mechanical Chest Compression Devices over Manual Cardiopulmonary Resuscitation: A Systematic Review with Meta-analysis and Trial Sequential Analysis.West J Emerg Med. 2021 Jul 19;22(4):810-819. doi: 10.5811/westjem.2021.3.50932. West J Emerg Med. 2021. PMID: 35353993 Free PMC article.
-
Mechanical CPR devices compared to manual CPR during out-of-hospital cardiac arrest and ambulance transport: a systematic review.Scand J Trauma Resusc Emerg Med. 2012 Jun 18;20:39. doi: 10.1186/1757-7241-20-39. Scand J Trauma Resusc Emerg Med. 2012. PMID: 22709917 Free PMC article.
Cited by
-
Comparison of in-hospital use of mechanical chest compression devices for out-of-hospital cardiac arrest patients: AUTOPULSE vs LUCAS.Medicine (Baltimore). 2019 Nov;98(45):e17881. doi: 10.1097/MD.0000000000017881. Medicine (Baltimore). 2019. PMID: 31702660 Free PMC article.
-
Efficacy and safety of mechanical versus manual compression in cardiac arrest - A Bayesian network meta-analysis.Resuscitation. 2018 Sep;130:182-188. doi: 10.1016/j.resuscitation.2018.05.005. Epub 2018 May 7. Resuscitation. 2018. PMID: 29746986 Free PMC article. Review.
-
The association between mechanical CPR and outcomes from in-hospital cardiac arrest: An observational cohort study.Resuscitation. 2024 May;198:110142. doi: 10.1016/j.resuscitation.2024.110142. Epub 2024 Feb 10. Resuscitation. 2024. PMID: 38342294 Free PMC article.
-
Comparison between manual and mechanical chest compressions during resuscitation in a pediatric animal model of asphyxial cardiac arrest.PLoS One. 2017 Nov 30;12(11):e0188846. doi: 10.1371/journal.pone.0188846. eCollection 2017. PLoS One. 2017. PMID: 29190801 Free PMC article.
-
Comparison between automated cardiopulmonary resuscitation and manual cardiopulmonary resuscitation in the rescue of cardiac and respiratory arrest.Pak J Med Sci. 2022 Nov-Dec;38(8):2208-2214. doi: 10.12669/pjms.38.8.6598. Pak J Med Sci. 2022. PMID: 36415278 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
