

doi: 10.4103/0366-6999.173525.
Malposition of Central Venous Catheter: Presentation and Management
Affiliations
- PMID: 26830995
- PMCID: PMC4799551
- DOI: 10.4103/0366-6999.173525
Item in Clipboard
Malposition of Central Venous Catheter: Presentation and Management
Chin Med J (Engl).
.
No abstract available
Figures
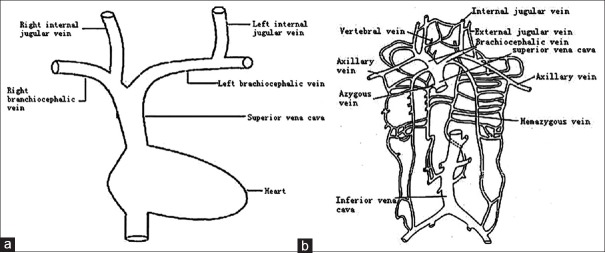
(a) The trunk of the superior vena cava system. It shows that left internal jugular vein negotiates two 90° turns. (b) Tributaries of the superior vena cava system. It shows that the superior vena cava drains venous blood from the upper half of the body in which there would be variable and complicated considerably.
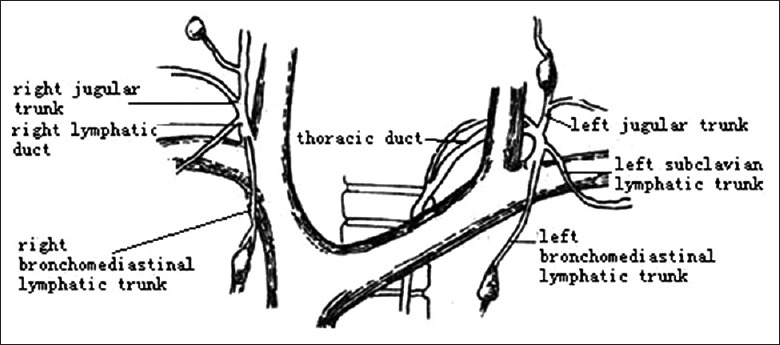
A anatomic illustration of the jugular lymphatic trunk. It indicates that the thoracic duct is medial close to the internal jugular vein in front of the internal jugular vein.

Catheter misplacement to intra-artery. (a) Chest film shows the tip of the catheter passing close to the aortic arch (arrow). (b) Further imaging indicates the tip of the catheter lying in the position of the arterial system (arrow).
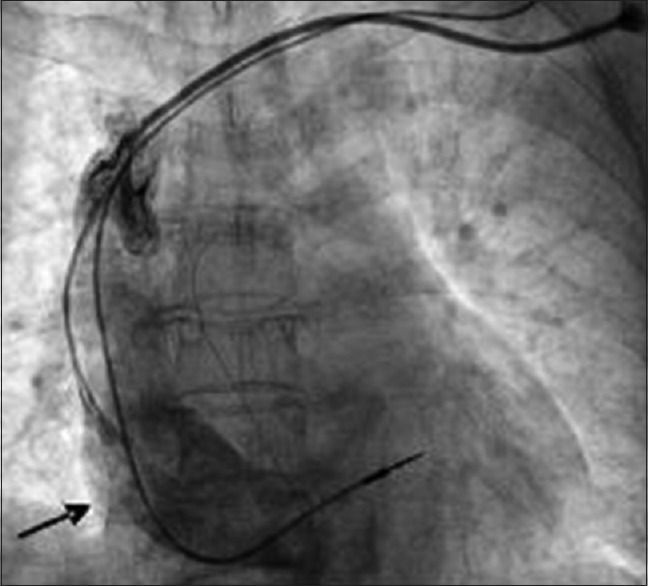
Chest film shows that the guide wire enters to azygos veins system through the left internal jugular vein during catheterization (arrow).
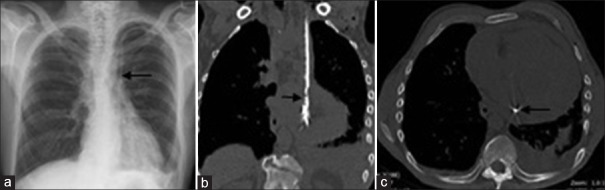
Catheter misplacement to the persistent left-sided SVC.[32] (a) The chest X-ray demonstrates that dialysis catheter passes down the left side of the mediastinum with pleural effusion and subcutaneous emphysema over the left clavicle (arrow). (b) Computed tomography chest demonstrates the catheter in the persistent left-sided SVC, pericardial and pleural effusion from coronal view (arrow). (c) The arrow indicates the catheter in the persistent left-sided SVC from conventional view. SVC: Superior vena cava.

Catheter misplacement to the right internal mammary vein.[33] (a) Chest X-ray: Anterior-posterior demonstrating what appears to be good position of catheter in the superior vena cava. (b) Computed tomography (axial image): Catheter malposition to the right of the sternum.

Catheter misplacement to the vertebral vein.[37] Chest X-ray shows that the central venous catheter passes the transverse processes of the 6th and the 7th cervical vertebrae (arrow).

The misplacement of a left internal jugular vein catheter. (a) The chest film shows both of lumens’ inadvertent insertion into the right internal jugular vein (arrow). (b) The chest film shows one of lumen dwelling into the right internal jugular vein (arrow).

Catheter misplacement to the subclavian vein.[39] Chest radiograph shows that the catheter is inserted via the right internal jugular vein and loops in the subclavian vein.

Catheter misplacement to the extradural space.[41] Cervical computed tomography scans demonstrate that the central venous catheter has penetrated the posterior aspect of the internal jugular vein. (a) Chest radiograph reveals that the tip of the central venous line (arrows) runs inside the normal route of the internal jugular vein and appears to overlap with the cervical spine (arrows). (b) The cervical computed tomography scan demonstrates that the catheter travels posterior to the carotid artery (arrows). (c) The cervical computed tomography scan shows that the catheter penetrates the prevertebral fascia (arrow). (d) The image indicates that the catheter enters the intervertebral foramen (arrow).

Catheter misplacement to the pericardium.[6] Chest radiograph reveals that the tip of the catheter is seen to lie within the right atrium (arrow).

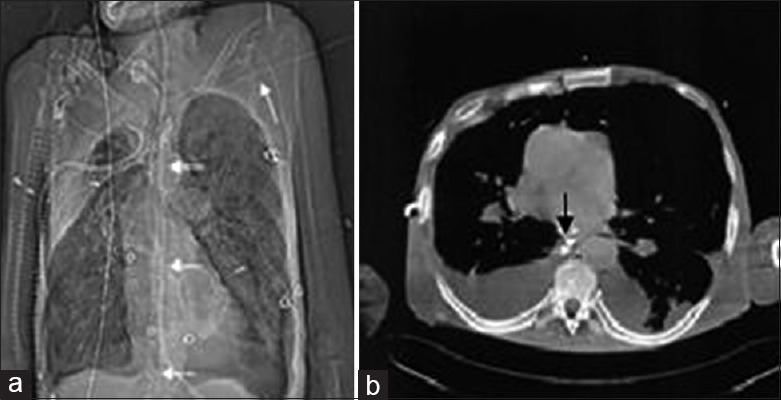
Catheter misplacement to the pleural space.[6] (a) The left-sided dialysis catheter has perforated through the right wall of SVC, and the tip has entered the right pleural space (arrow). (b) The left-sided dialysis catheter has perforated through the right wall of SVC and kink in the right pleural space (arrow). CVC: Central venous catheter; SVC: Superior vena cava.

Catheter misplacement to the mediastinum.[6] The computed tomography image shows the mediastinum grows for the huge hematoma. SVC: Superior vena cava.
Catheter misplacement to the thoracic duct.[44] (a) Scout view of the chest computed tomography shows the guidewire (arrows) takes a straight craniocaudal course projecting on the vertebral column reaching caudal to the diaphragm. (b) Computed tomography cross-sectional image at the level of the middle mediastinum. The guidewire (arrow) can be seen in a prevertebral position adjacent to the descending aorta and posterior to the esophagus.
Similar articles
-
Inadvertent cannulation of vertebral artery with a dialysis catheter.J Vasc Access. 2017 Sep 11;18(5):e71-e72. doi: 10.5301/jva.5000701. J Vasc Access. 2017. PMID: 28430312 No abstract available.
-
Hemodialysis catheter-induced stroke.J Vasc Access. 2014 Jul-Aug;15(4):325-6. doi: 10.5301/jva.5000193. Epub 2013 Oct 7. J Vasc Access. 2014. PMID: 24101421 No abstract available.
-
Removal of tunneled-cuffed catheters in children: is it safe to leave the cuff?J Vasc Access. 2017 Mar 21;18(2):e22-e23. doi: 10.5301/jva.5000653. J Vasc Access. 2017. PMID: 28165576 No abstract available.
-
Malposition of a central venous catheter into the right internal mammary vein: review of complications of catheter misplacement.Vasc Endovascular Surg. 2012 Feb;46(2):187-9. doi: 10.1177/1538574411433288. Epub 2012 Feb 5. Vasc Endovascular Surg. 2012. PMID: 22308215 Review.
-
Central venous catheters.BMJ. 2013 Nov 11;347:f6570. doi: 10.1136/bmj.f6570. BMJ. 2013. PMID: 24217269 Review. No abstract available.
Cited by
-
Utilizing the Retrograde Descending Internal Mammary Vein in DIEP Flap Anastomosis.Eplasty. 2018 Oct 29;18:ic23. eCollection 2018. Eplasty. 2018. PMID: 30455783 Free PMC article. No abstract available.
-
Rare Central Venous Catheter Malpositions: A Case Series.Cureus. 2024 Jul 4;16(7):e63872. doi: 10.7759/cureus.63872. eCollection 2024 Jul. Cureus. 2024. PMID: 38974401 Free PMC article.
-
Central Venous Line Insertion Revealing Partial Anomalous Pulmonary Venous Return: Diagnosis and Management.Case Rep Crit Care. 2017;2017:3218063. doi: 10.1155/2017/3218063. Epub 2017 May 29. Case Rep Crit Care. 2017. PMID: 28634556 Free PMC article.
-
Case Report of a Left-sided Superior Vena Cava Causing Unique Positioning of Central Line.Clin Pract Cases Emerg Med. 2020 Nov;4(4):587-590. doi: 10.5811/cpcem.2020.8.48372. Clin Pract Cases Emerg Med. 2020. PMID: 33217279 Free PMC article.
-
Straight to the back: Femoral triple lumen catheter misplaced in a lumbar vein.Radiol Case Rep. 2025 May 29;20(8):4082-4086. doi: 10.1016/j.radcr.2025.04.122. eCollection 2025 Aug. Radiol Case Rep. 2025. PMID: 40519848 Free PMC article.
References
-
- Tan PL, Gibson M. Central venous catheters: The role of radiology. Clin Radiol. 2006;61:13–22. - PubMed
-
- Trerotola SO, Kuhn-Fulton J, Johnson MS, Shah H, Ambrosius WT, Kneebone PH. Tunneled infusion catheters: Increased incidence of symptomatic venous thrombosis after subclavian versus internal jugular venous access. Radiology. 2000;217:89–93. - PubMed
-
- Bourquelot P. Vascular access for haemodialysis. Nephrol Ther. 2009;5:239–48. doi: 10.1016/j.nephro.2009.02.003. - PubMed
-
- Ruesch S, Walder B, Tramèr MR. Complications of central venous catheters: Internal jugular versus subclavian access – A systematic review. Crit Care Med. 2002;30:454–60. - PubMed
-
- Shannon D. Central venous catheter-induced pericardial effusion in a neonate: A case study and recommendations for practice. Neonatal Netw. 2014;33:341–8. doi: 10.1891/0730-0832.33.6.341. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
