

Utilizing Remote Real-Time Videoconferencing to Expand Access to Cancer Genetic Services in Community Practices: A Multicenter Feasibility Study
- PMID: 26831751
- PMCID: PMC4754531
- DOI: 10.2196/jmir.4564
Utilizing Remote Real-Time Videoconferencing to Expand Access to Cancer Genetic Services in Community Practices: A Multicenter Feasibility Study
Abstract
Background: Videoconferencing has been used to expand medical services to low-access populations and could increase access to genetic services at community sites where in-person visits with genetic providers are not available.
Objective: To evaluate the feasibility of, patient feedback of, and cognitive and affective responses to remote two-way videoconferencing (RVC) telegenetic services at multiple sociodemographically diverse community practices without access to genetic providers.
Methods: Patients at 3 community sites in 2 US states outside the host center completed RVC pretest (visit 1, V1) and post-test (visit 2, V2) genetic counseling for cancer susceptibility. Surveys evaluated patient experiences, knowledge, satisfaction with telegenetic and cancer genetics services, anxiety, depression, and cancer worry.
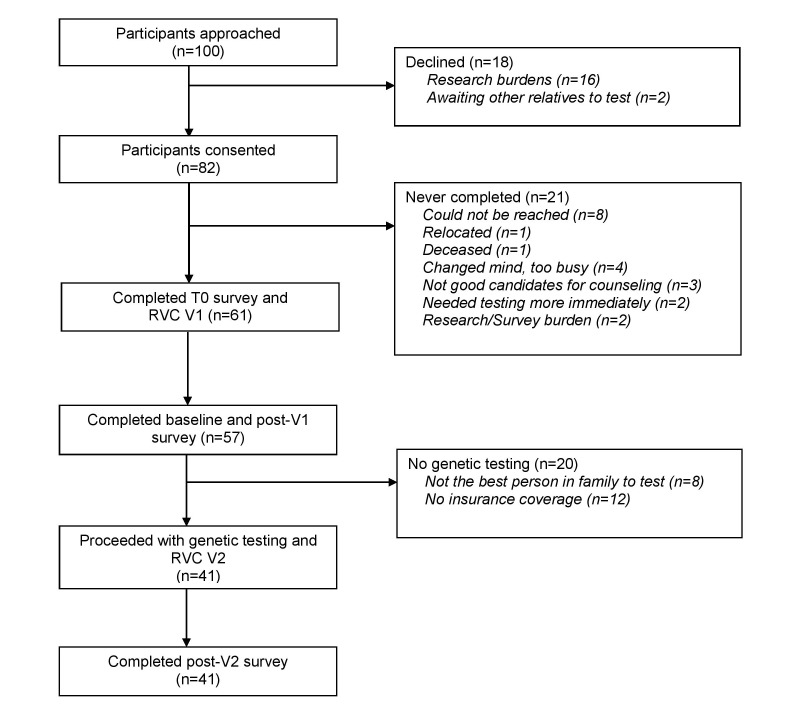
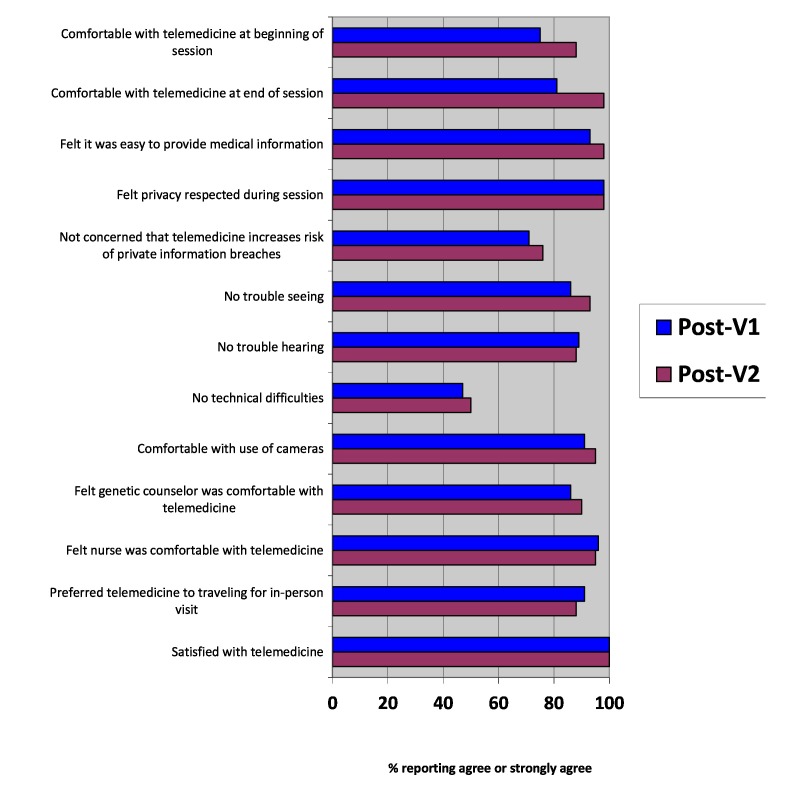
Results: A total of 82 out of 100 (82.0%) approached patients consented to RVC services. A total of 61 out of 82 patients (74%) completed pretest counseling and 41 out of 61 (67%) proceeded with testing and post-test counseling. A total of 4 out of 41 (10%) mutation carriers were identified: BRCA2, MSH2, and PMS2. Patients reported many advantages (eg, lower travel burden and convenience) and few disadvantages to RVC telegenetic services. Most patients reported feeling comfortable with the video camera--post-V1: 52/57 (91%); post-V2: 39/41 (95%)--and that their privacy was respected--post-V1: 56/57 (98%); post-V2: 40/41 (98%); however, some reported concerns that RVC might increase the risk of a confidentiality breach of their health information--post-V1: 14/57 (25%); post-V2: 12/41 (29%). While the majority of patients reported having no trouble seeing or hearing the genetic counselor--post-V1: 47/57 (82%); post-V2: 39/41 (95%)--51 out of 98 (52%) patients reported technical difficulties. Nonetheless, all patients reported being satisfied with genetic services. Compared to baseline, knowledge increased significantly after pretest counseling (+1.11 mean score, P=.005); satisfaction with telegenetic (+1.74 mean score, P=.02) and genetic services (+2.22 mean score, P=.001) increased after post-test counseling. General anxiety and depression decreased after pretest (-0.97 mean anxiety score, P=.003; -0.37 mean depression score, P=.046) and post-test counseling (-1.13 mean anxiety score, P=.003; -0.75 mean depression score, P=.01); state anxiety and cancer-specific worry did not significantly increase.
Conclusions: Remote videoconferencing telegenetic services are feasible, identify genetic carriers in community practices, and are associated with high patient satisfaction and favorable cognitive and affective outcomes, suggesting an innovative delivery model for further study to improve access to genetic providers and services. Potential barriers to dissemination include technology costs, unclear billing and reimbursement, and state requirements for provider licensure.
Keywords: cancer genetics; dissemination and implementation; genetic counseling; genetic testing; health care delivery; telemedicine.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- U.S. Preventive Services Task Force Genetic risk assessment and BRCA mutation testing for breast and ovarian cancer susceptibility: Recommendation statement. Ann Intern Med. 2005 Sep 6;143(5):355–361. Erratum in Ann Intern Med. 2005 Oct 4;143(7):547.143/5/355 - PubMed
-
- Cancer Program Standards 2012: Ensuring Patient-Centered Care. Version 1.2.1. Chicago, IL: American College of Surgeons; 2012. [2015-12-18]. https://www.facs.org/~/media/files/quality%20programs/cancer/coc/program... .
-
- Anderson B, McLosky J, Wasilevich E, Lyon-Callo S, Duquette D, Copeland G. Barriers and facilitators for utilization of genetic counseling and risk assessment services in young female breast cancer survivors. J Cancer Epidemiol. 2012;2012:298745. doi: 10.1155/2012/298745. doi: 10.1155/2012/298745. - DOI - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
