

Usual Care for Adolescent Depression From Symptom Identification Through Treatment Initiation
- PMID: 26832387
- PMCID: PMC5541862
- DOI: 10.1001/jamapediatrics.2015.4158
Usual Care for Adolescent Depression From Symptom Identification Through Treatment Initiation
Abstract
Importance: Published guidelines describing effective adolescent depression care in primary care settings include screening, assessment, treatment initiation, and symptom monitoring. It is unclear the extent to which these steps are documented in patient health records.
Objective: To determine rates of appropriate follow-up care for adolescents with newly identified depression symptoms in 3 large health systems.
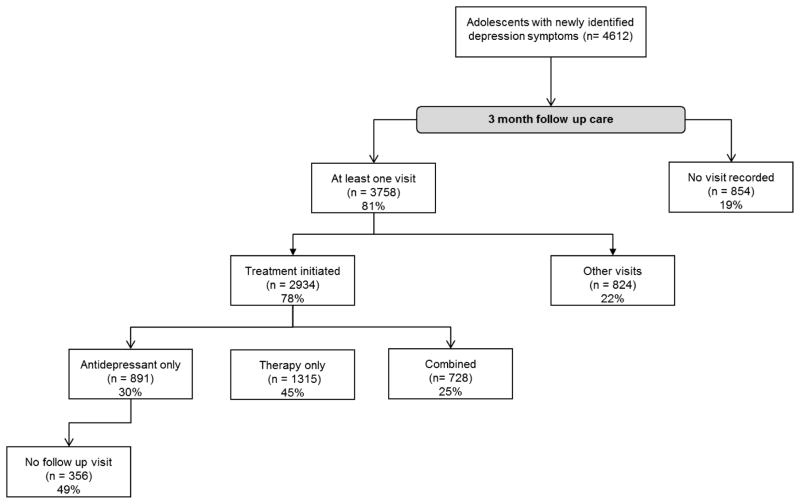
Design, setting, and participants: In this analysis conducted from March to September 2014, structured data retrospectively extracted from electronic health records were analyzed for 3 months following initial symptom identification to determine whether the patient was followed up and, if so, whether treatment was initiated and/or symptoms were monitored. Records were collected from 2 large health maintenance organizations in the western United States and a network of community health centers in the Northeast. The study group included adolescents (N = 4612) with newly identified depression symptoms, defined as an elevated score on the Patient Health Questionnaire (≥ 10) and/or a diagnosis of depression.
Main outcomes and measures: Rates of treatment initiation, symptom monitoring, and follow-up care documented within 3 months of initial symptom identification.
Results: Among the 4612 participants, the mean (SD) age at index event was 16.0 (2.3) years, and 3060 were female (66%). Treatment was initiated for nearly two-thirds of adolescents (79% of those with a diagnosis of major depression; n = 023); most received psychotherapy alone or in combination with medications. However, in the 3 months following identification, 36% of adolescents received no treatment (n = 1678), 68% did not have a follow-up symptom assessment (n = 3136), and 19% did not receive any follow-up care (n = 854). Further, 40% of adolescents prescribed antidepressant medication did not have any documentation of follow-up care for 3 months (n = 356). Younger age (ages 15-17 years: odds ratio [OR], 0.78; 95% CI, 0.67-0.92 and ages 18-20 years: OR, 0.83; 95% CI, 0.70-0.99; P = .008), more severe initial symptoms (moderate: OR, 0.99; 95% CI, 0.82-1.21; moderate to severe: OR, 1.46; 95% CI, 1.19-1.80; and severe: OR, 2.14; 95% CI, 1.65-2.79; P < .001), and receiving a diagnosis (major depression/dysthymia: OR, 2.65; 95% CI, 2.20-3.20 and unspecified depression/adjustment disorder: OR, 1.75; 95% CI, 1.43-2.14; P < .001) were significantly associated with treatment initiation. Differences in rates of follow-up care were evident between sites (site 2: OR, 1.77; 95% CI, 1.45-2.16 and site 3: OR, 2.10; 95% CI, 1.72-2.57), suggesting that differences within health systems may also affect care received.
Conclusions and relevance: Most adolescents with newly identified depression symptoms received some treatment, usually including psychotherapy, within the first 3 months after identification. However, follow-up care was low and substantial variation existed between sites. These results raise concerns about the quality of care for adolescent depression.
Figures
Comment in
-
Pediatric Quality Measures.JAMA Pediatr. 2016 Apr;170(4):380. doi: 10.1001/jamapediatrics.2016.0005. JAMA Pediatr. 2016. PMID: 26832173 No abstract available.
References
-
- Substance Abuse and Mental Health Services Administration. Results from the 2012 National Survey on Drug Use and Health. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration; 2013. Mental Health Findings NSDUH series H-42, HHS publication no.(SMA) 11-4667.
-
- Eaton DK, Kann L, Kinchen S, Shanklin S, Ross J, Hawkins J, Harris WA, Lowry R, McManus T, Chyen D, Lim C, Whittle L, Brener ND, Wechsler H. Youth risk behavior surveillance - United States, 2009. MMWR Surveill Summ. 2010;59(5):1–142. - PubMed
-
- Weissman MM, Wolk S, Goldstein RB, Moreau D, Adams P, Greenwald S, Klier CM, Ryan ND, Dahl RE, Wickramaratne P. Depressed adolescents grown up. JAMA. 1999;281(18):1707–1713. - PubMed
-
- Lewinsohn PM, Hops H, Roberts RE, Seeley JR, Andrews JA. Adolescent psychopathology: I. Prevalence and incidence of depression and other DSM-III-R disorders in high school students. J Abnorm Psychol. 1993;102(1):133–144. - PubMed
-
- Merikangas KR, He JP, Burstein M, Swanson SA, Avenevoli S, Cui L, Benjet C, Georgiades K, Swendsen J. Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication--Adolescent Supplement (NCS-A) J Am Acad Child Adolesc Psychiatry. 2010;49(10):980–989. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
