

Guidelines on vitamin D replacement in bariatric surgery: Identification and systematic appraisal
- PMID: 26833101
- PMCID: PMC4792722
- DOI: 10.1016/j.metabol.2015.12.013
Guidelines on vitamin D replacement in bariatric surgery: Identification and systematic appraisal
Abstract
Introduction: Bariatric surgery is the most effective therapeutic option to reduce weight in morbidly obese individuals, but it results in a number of mineral and vitamin deficiencies. Clinical Practice Guidelines (CPGs) attempt to balance those benefits and harms to provide guidance to physicians and patients.
Objectives: We compare and evaluate the quality of the evidence and of the development process of current CPGs that provide recommendations on vitamin D replacement in patients undergoing bariatric surgery, using a validated tool.
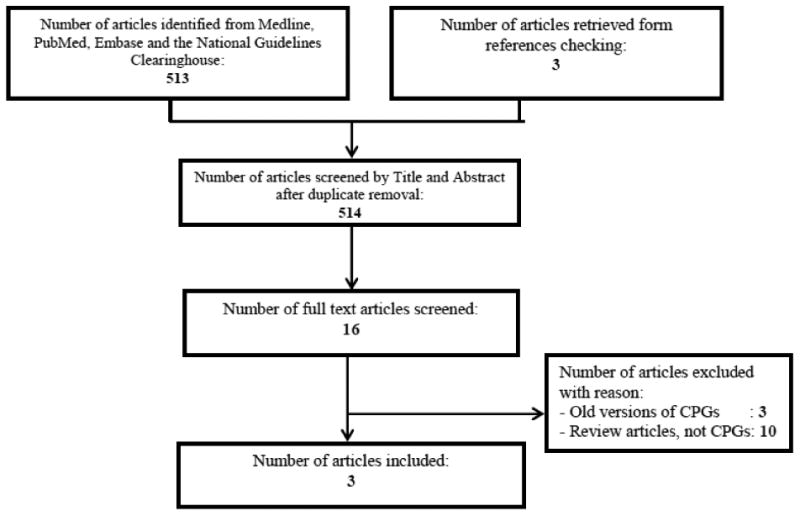
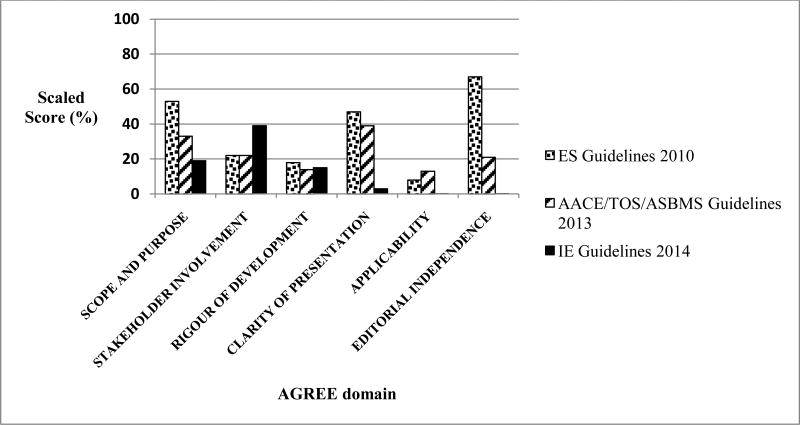
Methods: We searched 4 databases, with no time restriction, to identify relevant and current CPGs. Two reviewers assessed eligibility and abstracted data, in duplicate. They evaluated the quality of CPGs development process using the Appraisal of Guidelines, Research, and Evaluation II (AGREE II) tool that consists of 6 domains. A content expert verified those assessments.
Results: We identified 3 eligible CPGs: (1) the Endocrine Society (ES) guidelines (2010); (2) the American Association of Clinical Endocrinologists (AACE), The Obesity Society (TOS), and the American Society for Metabolic & Bariatric Surgery (ASMBS) guidelines (update 2013); and (3) the Interdisciplinary European (IE) guidelines on Metabolic and Bariatric Surgery (latest update 2014). The ES and the AACE/TOS/ASMBS guidelines recommended high doses of vitamin D, varying from 3000IU daily to 50,000IU 1-3 times weekly. Vitamin D doses were not mentioned in the IE guidelines. The recommendations were based on a low quality of evidence, if any, or limited to a single high quality trial, for some outcomes. In terms of quality, only the IE guidelines described their search methodology but none of the CPGs provided details on evidence selection and appraisal. None of the three CPGs rigorously assessed the preferences of the target population, resource implications, and the applicability of these guidelines. According to the AGREE II tool, we rated the ES guidelines as average in quality, and the other two as low in quality.
Conclusion: Current CPGs recommendations on vitamin D supplementation in bariatric surgery differ between societies. They do not fulfill criteria for optimal guideline development, in part possibly due to limited resources, and are based on expert opinion. Thus, the pressing need for high quality randomized trials to inform CPGs, to be developed based on recommended standards.
Keywords: Appraisal tool; Bariatric surgery; Clinical practice guidelines; Quality of evidence; Vitamin D replacement.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
References
-
- McTigue KM, Harris R, Hemphill B, Lux L, Sutton S, Bunton AJ, et al. Screening and interventions for obesity in adults: summary of the evidence for the US Preventive Services Task Force. Ann Intern Med. 2003;139(11):933–49. - PubMed
-
- Cole AJ, Beckman LM, Earthman CP. Vitamin D Status Following Bariatric Surgery: Implications and Recommendations. Nutr Clin Pract. 2014;29(6):751–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
