

Prediction of Fluoroquinolone Resistance in Gram-Negative Bacteria Causing Bloodstream Infections
- PMID: 26833166
- PMCID: PMC4808151
- DOI: 10.1128/AAC.02728-15
Prediction of Fluoroquinolone Resistance in Gram-Negative Bacteria Causing Bloodstream Infections
Abstract
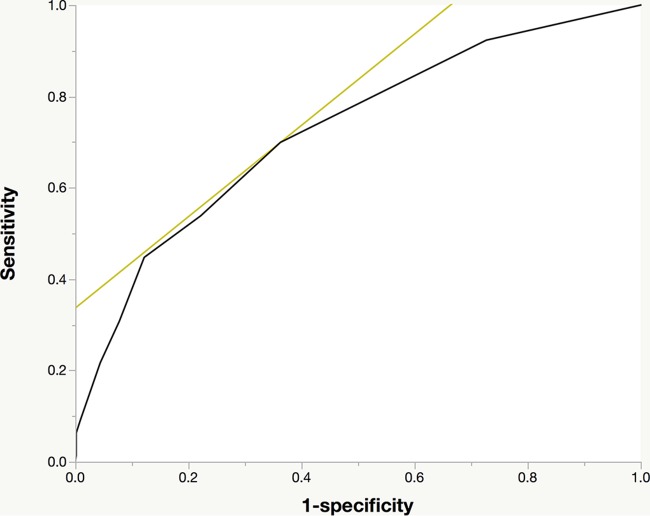
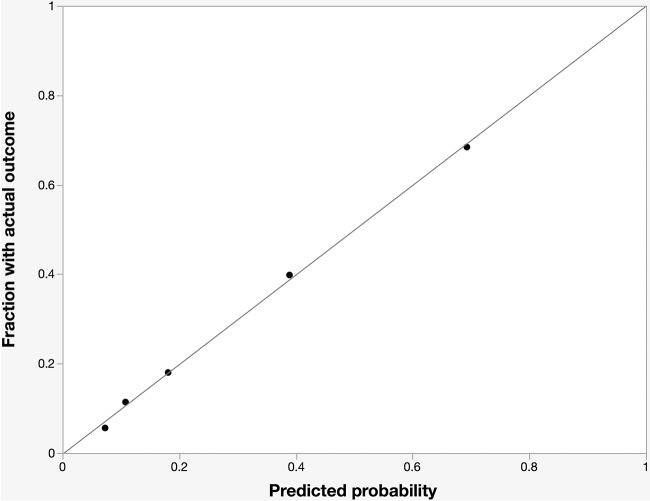
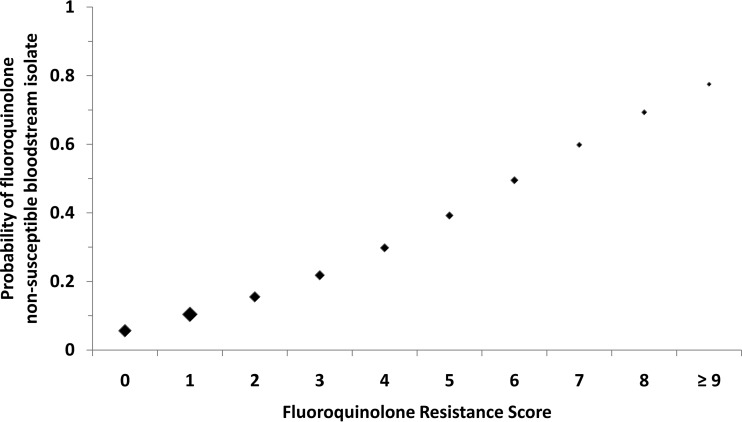
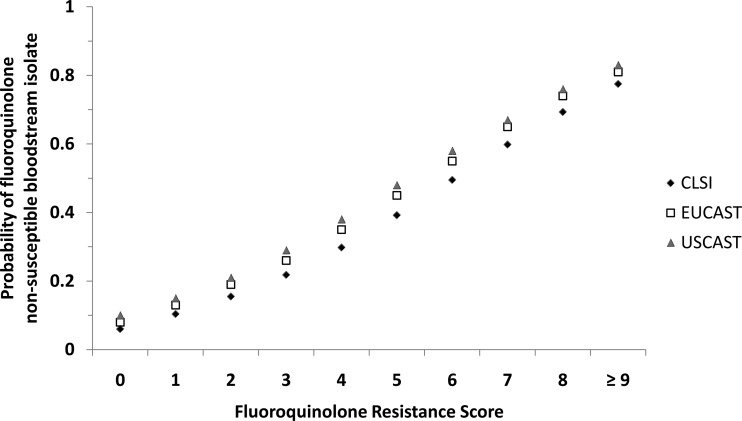
Increasing rates of fluoroquinolone resistance (FQ-R) have limited empirical treatment options for Gram-negative infections, particularly in patients with severe beta-lactam allergy. This case-control study aims to develop a clinical risk score to predict the probability of FQ-R in Gram-negative bloodstream isolates. Adult patients with Gram-negative bloodstream infections (BSI) hospitalized at Palmetto Health System in Columbia, South Carolina, from 2010 to 2013 were identified. Multivariate logistic regression was used to identify independent risk factors for FQ-R. Point allocation in the fluoroquinolone resistance score (FQRS) was based on regression coefficients. Model discrimination was assessed by the area under receiver operating characteristic curve (AUC). Among 824 patients with Gram-negative BSI, 143 (17%) had BSI due to fluoroquinolone-nonsusceptible Gram-negative bacilli. Independent risk factors for FQ-R and point allocation in FQRS included male sex (adjusted odds ratio [aOR], 1.97; 95% confidence intervals [CI], 1.36 to 2.98; 1 point), diabetes mellitus (aOR, 1.54; 95% CI, 1.03 to 2.28; 1 point), residence at a skilled nursing facility (aOR, 2.28; 95% CI, 1.42 to 3.63; 2 points), outpatient procedure within 30 days (aOR, 3.68; 95% CI, 1.96 to 6.78; 3 points), prior fluoroquinolone use within 90 days (aOR, 7.87; 95% CI, 4.53 to 13.74; 5 points), or prior fluoroquinolone use within 91 to 180 days of BSI (aOR, 2.77; 95% CI, 1.17 to 6.16; 3 points). The AUC for both final logistic regression and FQRS models was 0.73. Patients with an FQRS of 0, 3, 5, or 8 had predicted probabilities of FQ-R of 6%, 22%, 39%, or 69%, respectively. The estimation of patient-specific risk of antimicrobial resistance using FQRS may improve empirical antimicrobial therapy and fluoroquinolone utilization in Gram-negative BSI.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Retamar P, Portillo MM, López-Prieto MD, Rodríguez-López F, de Cueto M, García MV, Gómez MJ, Del Arco A, Muñoz A, Sánchez-Porto A, Torres-Tortosa M, Martín-Aspas A, Arroyo A, García-Figueras C, Acosta F, Corzo JE, León-Ruiz L, Escobar-Lara T, Rodríguez-Baño J, SAEI/Bacteremia Group SAMPAC . 2012. Impact of inadequate empirical therapy on the mortality of patients with bloodstream infections: a propensity score-based analysis. Antimicrob Agents Chemother 56:472–478. doi:10.1128/AAC.00462-11. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
