

Tricuspid Regurgitation and Mortality in Patients With Transvenous Permanent Pacemaker Leads
- PMID: 26833208
- PMCID: PMC4775321
- DOI: 10.1016/j.amjcard.2015.12.038
Tricuspid Regurgitation and Mortality in Patients With Transvenous Permanent Pacemaker Leads
Abstract
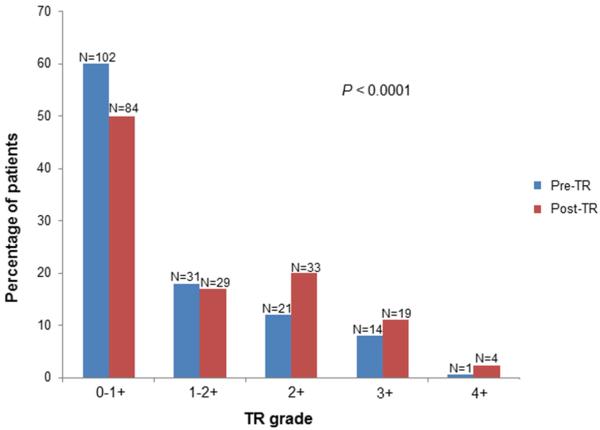
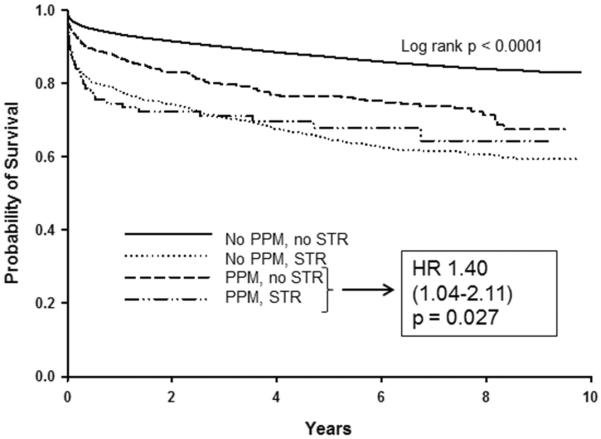
Estimates of the prevalence and importance of significant tricuspid regurgitation (STR) related to implantable device leads are based mainly on case reports, small observational studies, or mixed samples that include defibrillators. We sought to assess whether patients with permanent pacemaker (PPM) leads have an increased risk of STR and to determine mortality associated with PPM-related TR in a large longitudinal single-center cohort. We examined the prevalence of STR (defined as moderate-severe or ≥3+) among all echocardiograms performed from 2005 to 2011 excluding those with defibrillators. We then examined mortality risk according to the prevalence of PPM and STR after adjusting for cardiac co-morbidities, left ventricular systolic/diastolic function, and pulmonary artery hypertension. We screened 93,592 echocardiograms (1,245 with PPM) in 58,556 individual patients (634 with PPM). The prevalence of STR was higher in patients after PPM placement (mean age 79 ± 3 years; 54% men) compared with those without a PPM (adjusted odds ratio 2.32; 95% confidence interval [CI] 1.54 to 3.49; p <0.0001). Among patients with a PPM lead, the presence of STR was associated with increased mortality (adjusted hazard ratio 1.40; 95% CI 1.04 to 2.11, p = 0.027, vs no STR). Compared with having neither a PPM lead nor STR, adjusted hazard ratios for death were 2.13 (95% CI 1.93 to 2.34) for STR but no PPM, 1.04 (0.89 to 1.22) for PPM without STR, and 1.55 (1.13 to 2.14) for PPM with STR. In conclusion, in a sample comprising >58,000 individual patients, PPM leads are associated with higher risk of STR after adjustment for left ventricular systolic/diastolic function and pulmonary artery hypertension; similarly to STR from other cardiac pathologies, PPM-related STR is associated with increased mortality.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
References
-
- Agarwal S, Tuzcu EM, Rodriguez ER, Tan CD, Rodriguez LL, Kapadia SR. Interventional cardiology perspective of functional tricuspid regurgitation. Circ Cardiovasc Interv. 2009;2:565–573. - PubMed
-
- Nath J, Foster E, Heidenreich PA. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004;43:405–409. - PubMed
-
- Iskandar SB, Ann Jackson S, Fahrig S, Mechleb BK, Garcia ID. Tricuspid valve malfunction and ventricular pacemaker lead: Case report and review of the literature. Echocardiography. 2006;23:692–697. - PubMed
-
- Kucukarslan N, Kirilmaz A, Ulusoy E, Yokusoglu M, Gramatnikovski N, Ozal E, Tatar H. Tricuspid insufficiency does not increase early after permanent implantation of pacemaker leads. J Card Surg. 2006;21:391–394. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
