

To drain or not to drain in colorectal anastomosis: a meta-analysis
- PMID: 26833470
- PMCID: PMC4834107
- DOI: 10.1007/s00384-016-2509-6
To drain or not to drain in colorectal anastomosis: a meta-analysis
Abstract
Background: Currently, many surgeons place a prophylactic drain in the abdominal or pelvic cavity after colorectal anastomosis as a conventional treatment. However, some trials have demonstrated that this procedure may not be beneficial to the patients.
Objective: To determine whether prophylactic placement of a drain in colorectal anastomosis can reduce postoperative complications.
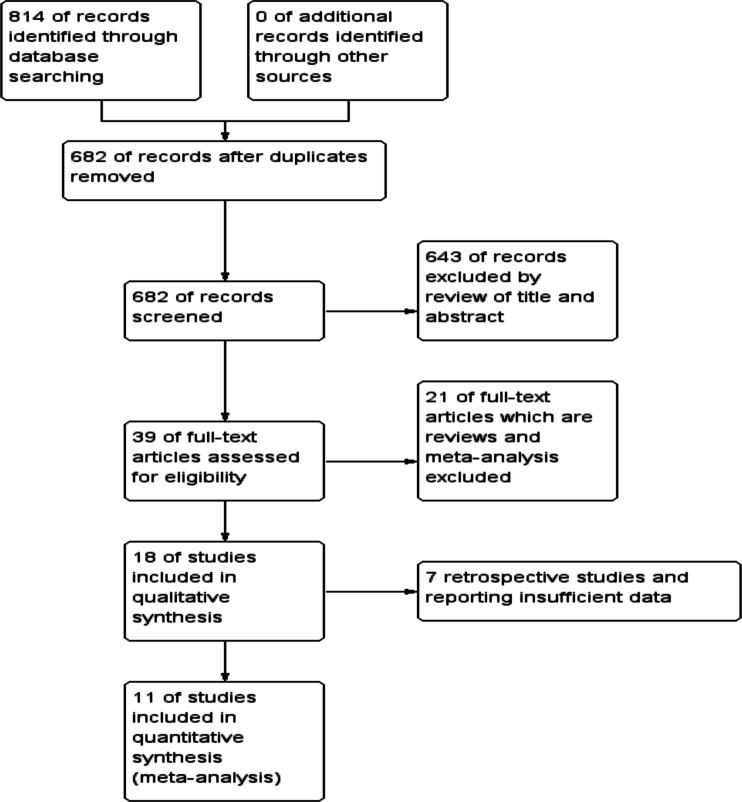
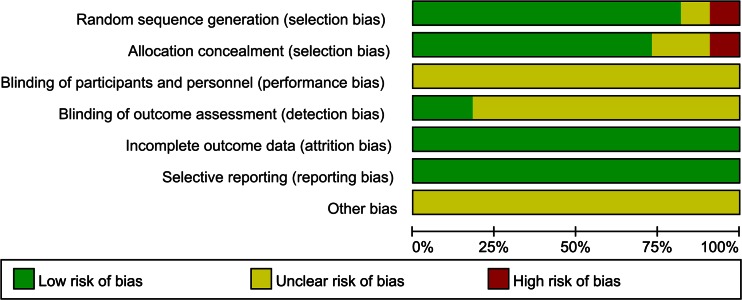
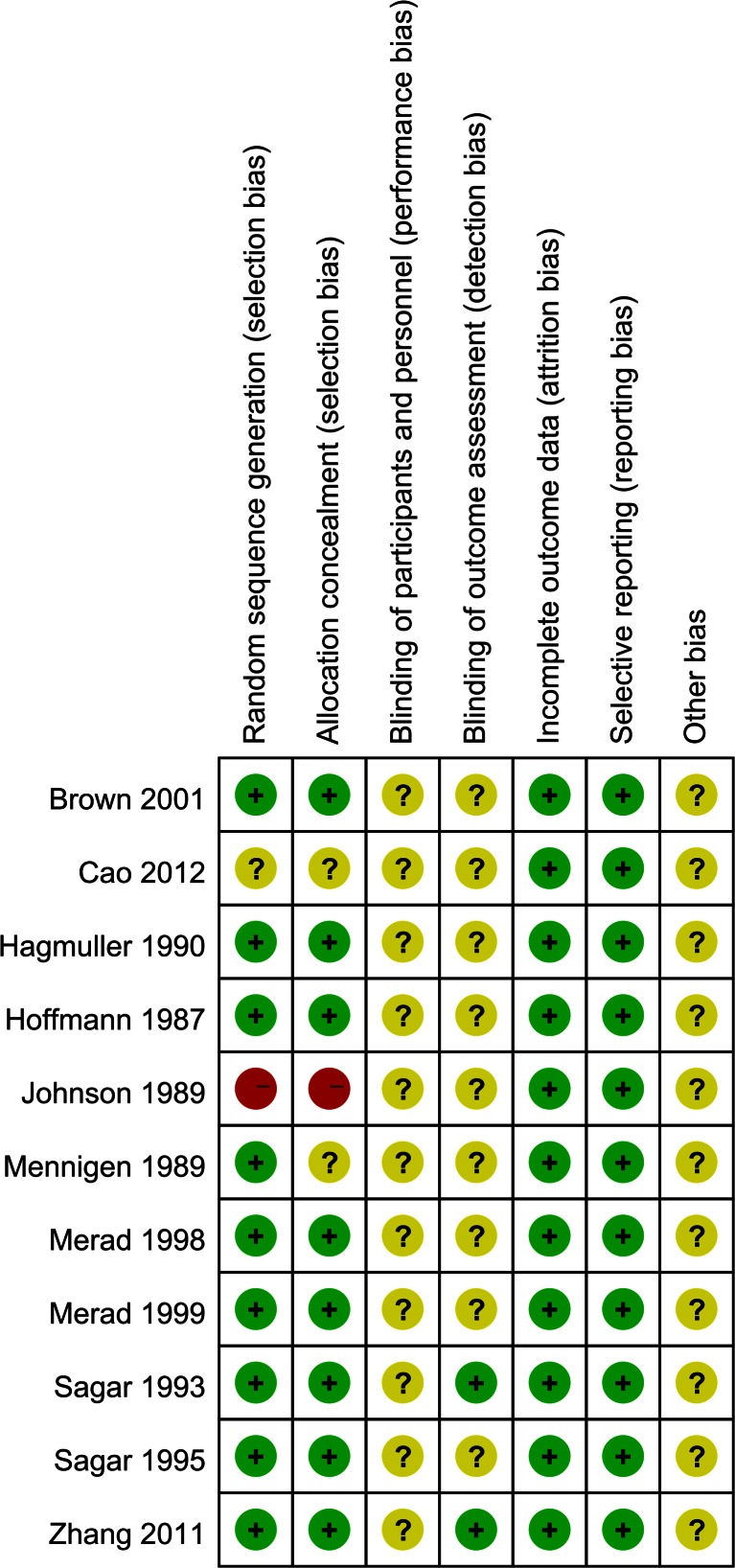
Methods: We systematically searched all the electronic databases for randomized controlled trials (RCTs) that compared routine use of drainage to non-drainage regimes after colorectal anastomosis, using the terms "colorectal" or "colon/colonic" or "rectum/rectal" and "anastomo*" and "drain or drainage." Reference lists of relevant articles, conference proceedings, and ongoing trial databases were also screened. Primary outcome measures were clinical and radiological anastomotic leakage. Secondary outcome measures included mortality, wound infection, re-operation, and respiratory complications. We assessed the eligible studies for risk of bias using the Cochrane Risk of Bias Tool. Two authors independently extracted data.
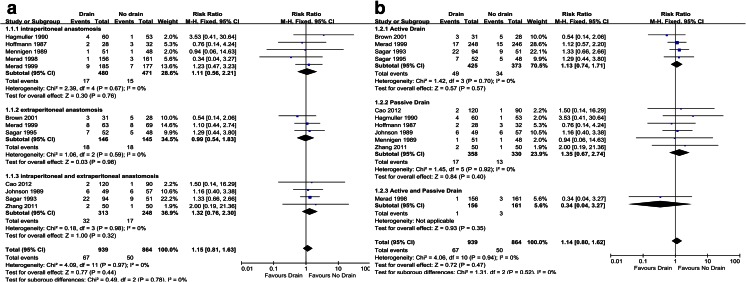
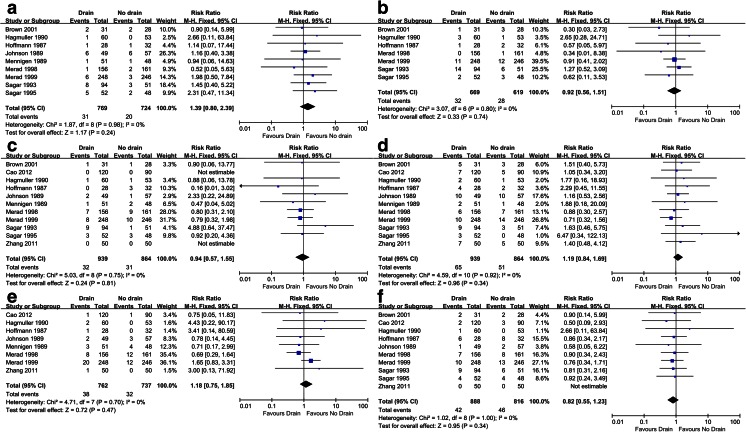
Results: Eleven RCTs were included (1803 patients in total, 939 patients in the drain group and 864 patients in the no drain group). Meta-analysis showed that there was no statistically significant differences between the drain group and the no drain group in (1) overall anastomotic leakage (relative risk (RR) = 1.14, 95 % confidence interval (CI) 0.80-1.62, P = 0.47), (2) clinical anastomotic leakage (RR = 1.39, 95 % CI 0.80-2.39, P = 0.24), (3) radiologic anastomotic leakage (RR = 0.92, 95 % CI 0.56-1.51, P = 0.74), (4) mortality (RR = 0.94, 95 % CI 0.57-1.55, P = 0.81), (5) wound infection (RR = 1.19, 95 % CI 0.84-1.69, P = 0.34), (6) re-operation (RR = 1.18, 95 % CI 0.75-1.85, P = 0.47), and (7) respiratory complications (RR = 0.82, 95 % CI 0.55-1.23, P = 0.34).
Conclusions: Routine use of prophylactic drainage in colorectal anastomosis does not benefit in decreasing postoperative complications.
Keywords: Colorectal anastomosis; Drain; Meta-analysis; Postoperative complications.
Figures
Similar articles
-
Colon and rectal anastomoses do not require routine drainage: a systematic review and meta-analysis.Ann Surg. 1999 Feb;229(2):174-80. doi: 10.1097/00000658-199902000-00003. Ann Surg. 1999. PMID: 10024097 Free PMC article.
-
Is a drain necessary after anterior resection of the rectum? A systematic review and meta-analysis.Int J Colorectal Dis. 2019 Jun;34(6):973-981. doi: 10.1007/s00384-019-03276-4. Epub 2019 Apr 25. Int J Colorectal Dis. 2019. PMID: 31025093
-
Prophylactic pelvic drainage after rectal resection with extraperitoneal anastomosis: is it worthwhile? A meta-analysis of randomized controlled trials.Int J Colorectal Dis. 2017 Nov;32(11):1531-1538. doi: 10.1007/s00384-017-2891-8. Epub 2017 Aug 24. Int J Colorectal Dis. 2017. PMID: 28840326
-
Prophylactic intra-abdominal drainage following colorectal anastomoses. A systematic review and meta-analysis of randomized controlled trials.Am J Surg. 2020 Jan;219(1):164-174. doi: 10.1016/j.amjsurg.2019.05.006. Epub 2019 May 22. Am J Surg. 2020. PMID: 31138400
-
Is prophylactic pelvic drainage useful after elective rectal or anal anastomosis? A multicenter controlled randomized trial. French Association for Surgical Research.Surgery. 1999 May;125(5):529-35. Surgery. 1999. PMID: 10330942 Clinical Trial.
Cited by
-
Abdominal drainage after elective colorectal surgery: propensity score-matched retrospective analysis of an Italian cohort.BJS Open. 2024 Jan 3;8(1):zrad107. doi: 10.1093/bjsopen/zrad107. BJS Open. 2024. PMID: 38170895 Free PMC article.
-
Optimized perioperative management (fast-track, ERAS) to enhance postoperative recovery in elective colorectal surgery.GMS Hyg Infect Control. 2022 Jun 23;17:Doc10. doi: 10.3205/dgkh000413. eCollection 2022. GMS Hyg Infect Control. 2022. PMID: 35909653 Free PMC article. Review.
-
Timing for removing prophylactic drains after liver resection: an evaluation of drain removal on the third and first postoperative days.Ann Transl Med. 2020 Apr;8(7):454. doi: 10.21037/atm.2020.04.04. Ann Transl Med. 2020. PMID: 32395498 Free PMC article.
-
Review of Colonic Anastomotic Leakage and Prevention Methods.J Clin Med. 2020 Dec 16;9(12):4061. doi: 10.3390/jcm9124061. J Clin Med. 2020. PMID: 33339209 Free PMC article. Review.
-
Attitudes towards Enhanced Recovery after Surgery (ERAS) interventions in colorectal surgery: nationwide survey of Australia and New Zealand colorectal surgeons.Langenbecks Arch Surg. 2022 Jun;407(4):1637-1646. doi: 10.1007/s00423-022-02488-7. Epub 2022 Mar 11. Langenbecks Arch Surg. 2022. PMID: 35275247 Free PMC article.
References
-
- Moss JP. Historical and current perspectives on surgical drainage. Surg Gynecol Obstet. 1981;152(4):517–527. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
