

Management of infantile spasms
- PMID: 26835388
- PMCID: PMC4728997
- DOI: 10.3978/j.issn.2224-4336.2015.09.01
Management of infantile spasms
Abstract
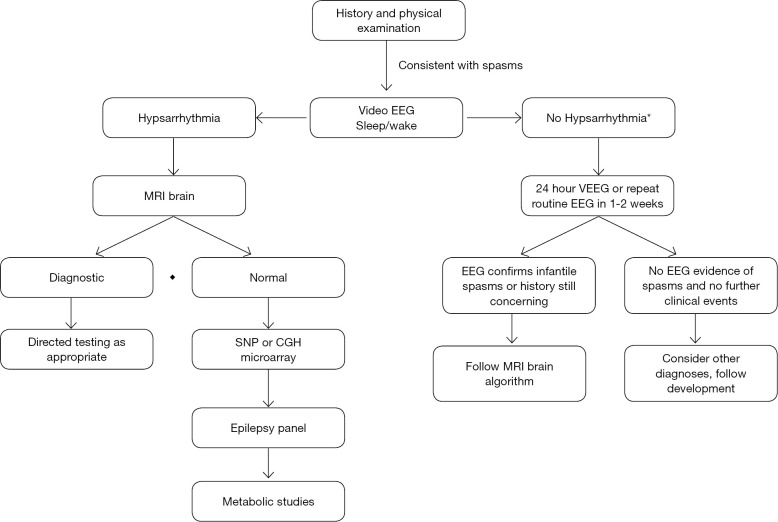
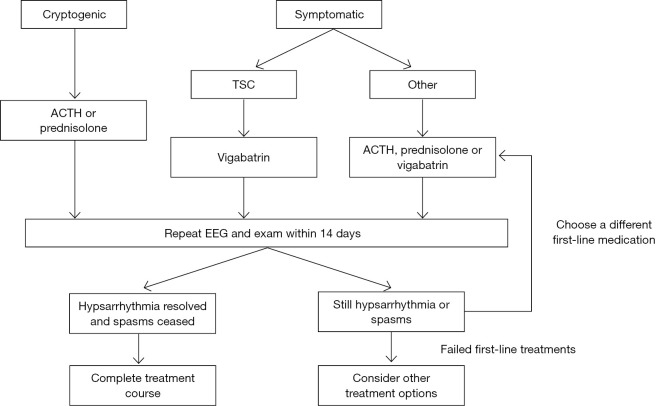
West syndrome, or infantile spasms syndrome is a frequently catastrophic infantile epileptic encephalopathy with a variety of etiologies. Despite the heterogeneous nature of causes of infantile spasms, a careful diagnostic evaluation can lead to diagnosis in many patients and may guide treatment choices. Magnetic resonance imaging (MRI) brain remains the highest yield initial study in determining the etiology in infantile spasms. Treatment of infantile spasms has little class I data, but adrenocorticotropic hormone (ACTH), prednisolone and vigabatrin have the best evidence as first-line medications. Other therapies including the ketogenic diet and other anti-epileptics medications may also prove useful in the treatment of infantile spasms. In general, more studies are needed to determine the best treatment regimen for this condition. Prognosis is generally poor, with the majority of patients having some or profound neurocognitive delays. Patients without delays at diagnosis and without an identifiable etiology, if treated appropriately, have the greatest likelihood of a normal outcome.
Keywords: Infantile spasms; West syndrome; adrenocorticotropic hormone (ACTH); corticosteroids; hypsarrhythmia.
Conflict of interest statement
Figures
References
-
- West WJ. On a peculiar form of infantile convulsions. Lancet 1841;1:724-5.
-
- Lux AL. West & son: the origins of West syndrome. Brain Dev 2001;23:443-6. - PubMed
-
- Pellock JM, Hrachovy R, Shinnar S, et al. Infantile spasms: a U.S. consensus report. Epilepsia 2010;51:2175-89. - PubMed
-
- Lux AL, Osborne JP. A proposal for case definitions and outcome measures in studies of infantile spasms and West syndrome: consensus statement of the West Delphi group. Epilepsia 2004;45:1416-28. - PubMed
Publication types
LinkOut - more resources
Full Text Sources