

Headache in a high school student - a reminder of fundamental principles of clinical medicine and common pitfalls of cognition
- PMID: 26835410
- PMCID: PMC4719433
- DOI: 10.5339/qmj.2015.15
Headache in a high school student - a reminder of fundamental principles of clinical medicine and common pitfalls of cognition
Abstract
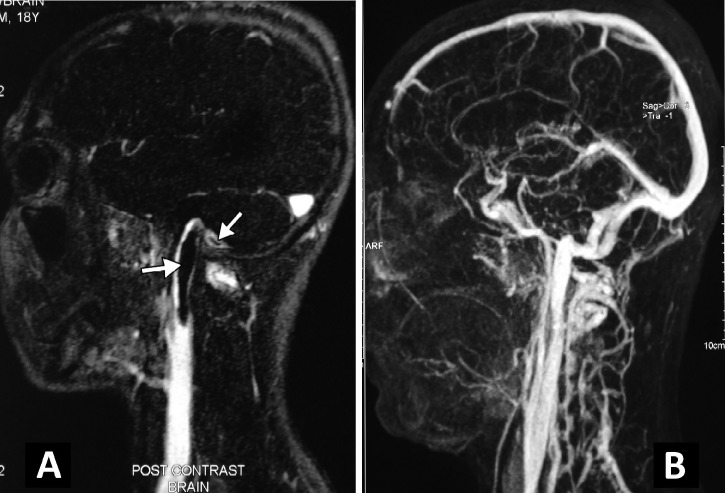
Primary headache disorders account for the majority of the cases of headache. Nevertheless, the primary objective of a physician, when encountered with a patient with headache is to rule out a secondary cause the headache. This entails a search for specific associated red-flag symptoms or signs that may indicate a serious condition, as well as a heightened suspicion of and evaluation for a don't miss diagnosis. We present a case of a high-school student whose first manifestation of systemic lupus erythematosus (SLE) was a headache due to cerebral venous and sinus thrombosis, initially misdiagnosed as tension-headache and 'ophthalmoplegic migraine' (now known as 'recurrent painful ophthalmoplegic neuropathy'). The patient made a complete neurological and radiological recovery after systemic anticoagulation and treatment of SLE. An analysis of the clinical errors and cognitive biases leading to delayed referral to hospital is presented. We highlight the fact that adherence to the fundamental principles of clinical medicine and enhancement of cognitive awareness is required to reduce diagnostic errors.
Keywords: Cerebral venous and sinus thrombosis; cognitive errors; headache; nephrotic syndrome; principles of clinical medicine; systemic lupus erythematosus.
Figures
Similar articles
-
Recurrent Painful Ophthalmoplegic Neuropathy Responding to Lamotrigine: A Case Report.Cureus. 2024 Mar 25;16(3):e56924. doi: 10.7759/cureus.56924. eCollection 2024 Mar. Cureus. 2024. PMID: 38665741 Free PMC article.
-
Cerebral Venous Sinus Thrombosis as a Rare Complication of Systemic Lupus Erythematosus: Subgroup Analysis of the VENOST Study.J Stroke Cerebrovasc Dis. 2019 Dec;28(12):104372. doi: 10.1016/j.jstrokecerebrovasdis.2019.104372. Epub 2019 Sep 24. J Stroke Cerebrovasc Dis. 2019. PMID: 31562041
-
[Psychiatric manifestations of lupus erythematosus systemic and Sjogren's syndrome].Encephale. 2001 Nov-Dec;27(6):588-99. Encephale. 2001. PMID: 11865567 French.
-
Posterior reversible encephalopathy syndrome--an underrecognized manifestation of systemic lupus erythematosus.J Rheumatol. 2006 Nov;33(11):2178-83. Epub 2006 Sep 1. J Rheumatol. 2006. PMID: 16960925 Review.
-
[Cerebral venous thrombosis in systemic lupus erythematosus. Case report and literature review].Rev Med Inst Mex Seguro Soc. 2006 Jul-Aug;44(4):365-9. Rev Med Inst Mex Seguro Soc. 2006. PMID: 16904040 Review. Spanish.
References
-
- Headache Classification Committee of the International Headache Society (IHS) The international classification of headache disorders, 3rd edition (beta version) Cephalalgia. 2013;33(9):629–808. - PubMed
-
- Soleau SW, Schmidt R, Stevens S, Osborn A, MacDonald JD. Extensive experience with dural sinus thrombosis. Neurosurgery. 2003;52:534–544. - PubMed
-
- Bentley JN, Figueroa RE, Vender JR. From presentation to follow-up: Diagnosis and treatment of cerebral venous thrombosis. Neurosurg Focus. 2009;27(5):E41–E47. - PubMed
-
- Förderreuther S, Ruscheweyh R. From ophthalmoplegic migraine to cranial neuropathy. Curr Pain Headache Rep. 2015 Jun;19(6):21. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources