

Intra-Wound Antibiotics and Infection in Spine Fusion Surgery: A Report from Washington State's SCOAP-CERTAIN Collaborative
- PMID: 26835891
- PMCID: PMC4790200
- DOI: 10.1089/sur.2015.146
Intra-Wound Antibiotics and Infection in Spine Fusion Surgery: A Report from Washington State's SCOAP-CERTAIN Collaborative
Abstract
Background: Surgical site infection (SSI) after spine surgery is classified as a "never event" by the Centers for Medicare and Medicaid. Intra-wound antibiotics (IWA) have been proposed to reduce the incidence of SSI, but robust evidence to support its use is lacking.
Methods: Prospective cohort undergoing spine fusion at 20 Washington State hospitals (July 2011 to March 2014) participating in the Spine Surgical Care and Outcomes Assessment Program (Spine SCOAP) linked to a discharge tracking system. Patient, hospital, and operative factors associated with SSI and IWA use during index hospitalizations through 600 days were analyzed using a random effects logistic model (index), and a time-to-event analysis (follow-up) using Cox proportional hazards.
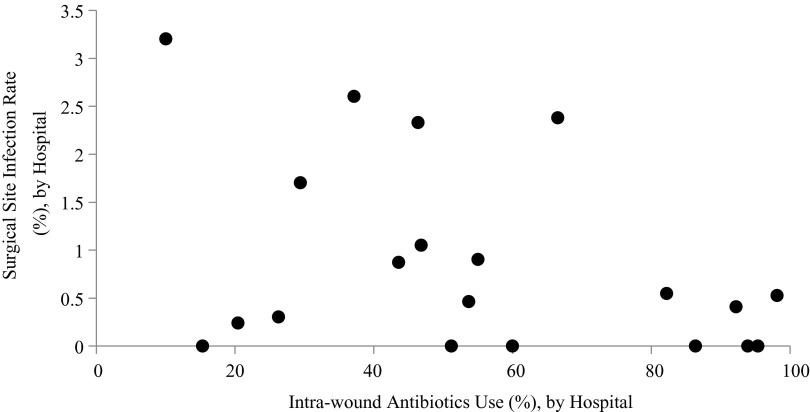
Results: A total of 9,823 patients underwent cervical (47%) or lumbar (53%) procedures (mean age, 58; 54% female) with an SSI rate of 1.1% during index hospitalization. Those with SSI were older, more often had diabetes mellitus, and more frequently underwent lumbar (versus cervical) fusion compared with those without SSI (all p < 0.01). Unadjusted rates of SSI during index hospitalization were lower in patients who received IWA (0.8% versus 1.5%). After adjustment for patient, hospital, and operative factors, no benefit was observed in those receiving IWA (odds ratio [OR] 0.65, 95% confidence interval [CI]: 0.42-1.03). At 12 mo, unadjusted rates of SSI were 2.4% and 3.0% for those who did and did not receive antibiotics; after adjustment there was no significant difference (hazard ratio [HR] 0.94, 95% CI: 0.62-1.42).
Conclusions: Whereas unadjusted analyses indicate a nearly 50% reduction in index SSI using IWA, we did not observe a statistically significant difference after adjustment. Despite its size, this study is underpowered to detect small but potentially relevant improvements in rates of SSI. It remains to be determined if IWA should be promoted as a quality improvement intervention. Concerns related to bias in the use of IWA suggest the benefit of a randomized trial.
Figures
References
-
- Weiss AJ, Elixhauser A. Trends in Operating Room Procedures in U.S. Hospitals, 2001–2011: Statistical Brief #171. Rockville, MD: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs, 2006
-
- Lee J. Rethinking spine care: Some health systems are moving beyond surgery in serving back pain patients. March 22, 2014. www.modernhealthcare.com/article/20140322/MAGAZINE/303229985 (Last accessed April8, 2015)
-
- Godil SS, Parker SL, O'Neill KR, et al. . Comparative effectiveness and cost-benefit analysis of local application of vancomycin powder in posterior spinal fusion for spine trauma: Clinical article. J Neurosurg Spine 2013;19:550–555 - PubMed
-
- Calderone RR, Garland DE, Capen DA, Oster H. Cost of medical care for postoperative spinal infections. Orthop Clin North Am 1996;27:171–182 - PubMed
-
- Miller A. Hospital reporting and “never events.” Medicare Patient Management 2009(May-Jun);4:20 www.medicarepatientmanagement.com/issues/04-03/mpmMJ09-NeverEvents.pdf (Last accessed April8, 2015)
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
