

Comparison of Recommendations in Clinical Practice Guidelines for Acute Gastroenteritis in Children
- PMID: 26835905
- PMCID: PMC6858859
- DOI: 10.1097/MPG.0000000000001133
Comparison of Recommendations in Clinical Practice Guidelines for Acute Gastroenteritis in Children
Abstract
Objective: Acute gastroenteritis (AGE) is a major cause of child mortality and morbidity. This study aimed at systematically reviewing clinical practice guidelines (CPGs) on AGE to compare recommendations and provide the basis for developing single universal guidelines.
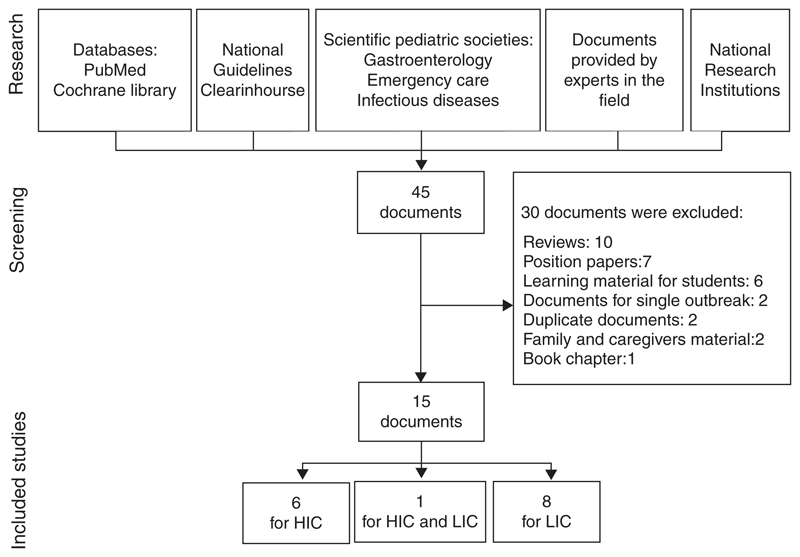
Methods: CPGs were identified by searching MEDLINE, Cochrane-Library, National Guideline Clearinghouse and Web sites of relevant societies/organizations producing and/or endorsing CPGs.
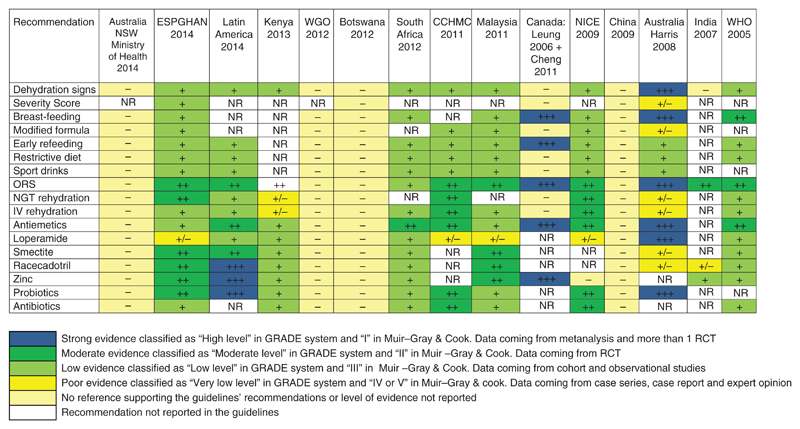
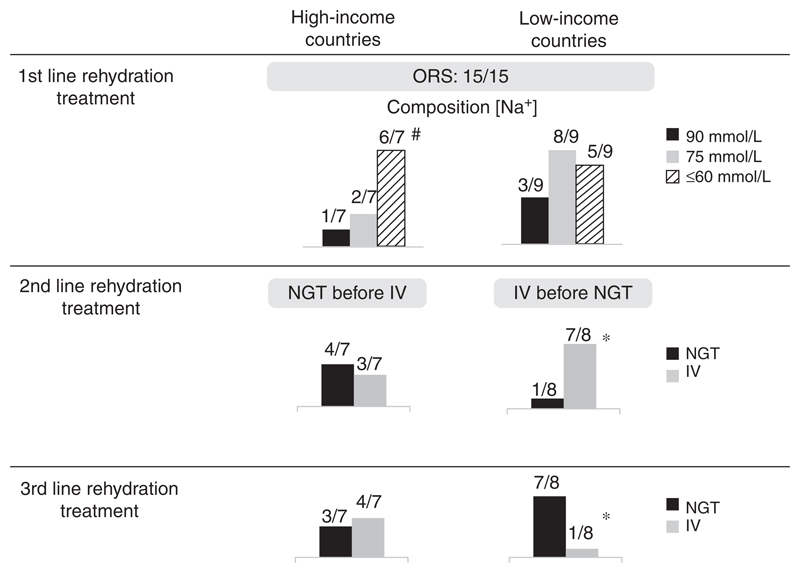
Results: The definition of AGE varies among the 15 CPGs identified. The parameters most frequently recommended to assess dehydration are skin turgor and sunken eyes (11/15, 73.3%), general appearance (11/15, 66.6%), capillary refill time, and mucous membranes appearance (9/15, 60%). Oral rehydration solution is universally recognized as first-line treatment. The majority of CPGs recommend hypo-osmolar (Na 45-60 mmol/L, 11/15, 66.6 %) or low-osmolality (Na 75 mmol/L, 9/15, 60%) solutions. In children who fail oral rehydration, most CPGs suggest intravenous rehydration (66.6%). However, nasogastric tube insertion for fluid administration is preferred according by 5/15 CPGs (33.3%). Changes in diet and withdrawal of food are discouraged by all CPGs, and early refeeding is strongly recommended in 13 of 15 (86.7%). Zinc is recommended as an adjunct to ORS by 10 of 15 (66.6%) CPGs, most of them from low-income countries. Probiotics are considered by 9 of 15 (60%) CPGs, 5 from high-income countries. Antiemetics are not recommended in 9 of 15 (60%) CPGs. Routine use of antibiotics is discouraged.
Conclusions: Key recommendations for the management of AGE in children are similar in CPGs. Together with accurate review of evidence-base this may represent a starting point for developing universal recommendations for the management of children with AGE worldwide.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Black RE, Cousens S, Johnson HL, et al. Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet. 2010;375:1969–87. - PubMed
-
- United Nations. The Millenium Development Goals Report 2014. UN, New York: 2014.
-
- Liu L, Johnson HL, Cousens S, et al. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379:2151–61. - PubMed
-
- United Nations. The Millennium Development Goals Report 2011. UN, New York: 2011.
-
- Quazi S, Aboubaker S, MacLean R, et al. Ending preventable child deaths from pneumonia and diarrhea by 2025. Development of the integrated Global Action Plan for the Prevention and Control of Pneumonia and Diarrhoea. Arch Dis Child. 2015;100:s23–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
