

Investigating the Radioresistant Properties of Lung Cancer Stem Cells in the Context of the Tumor Microenvironment
- PMID: 26836231
- PMCID: PMC4762254
- DOI: 10.1667/RR14285.1
Investigating the Radioresistant Properties of Lung Cancer Stem Cells in the Context of the Tumor Microenvironment
Abstract
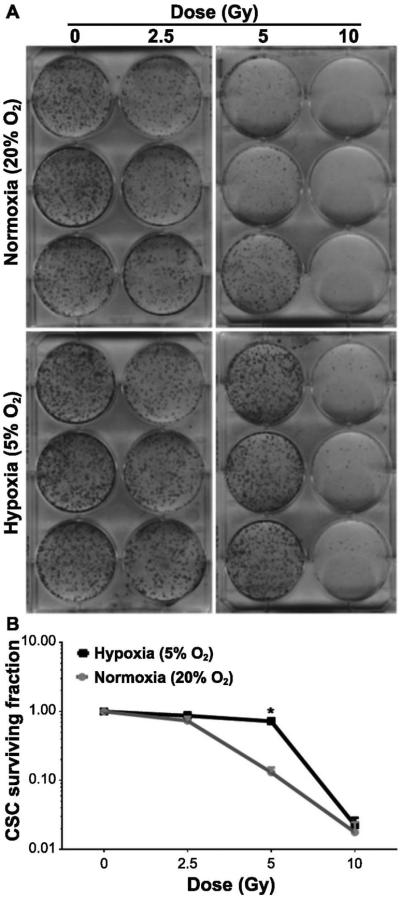
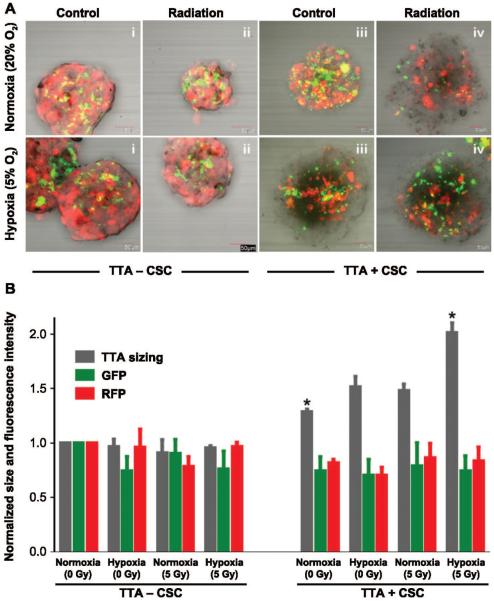
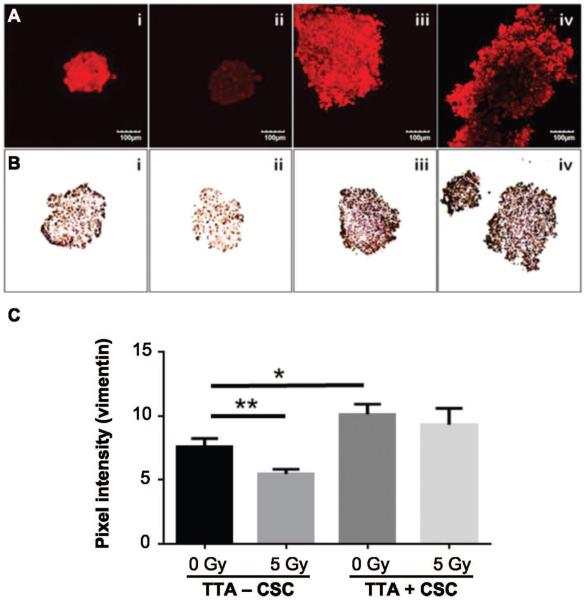
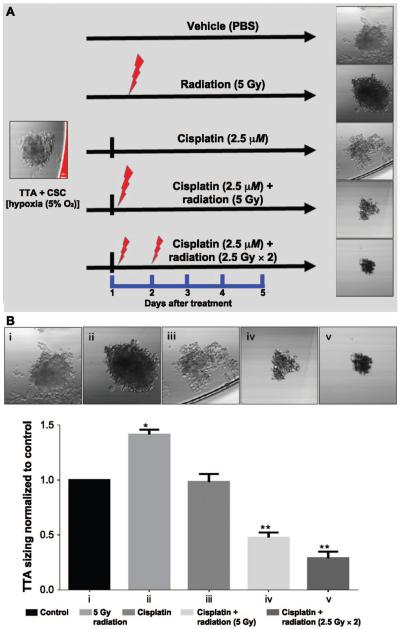
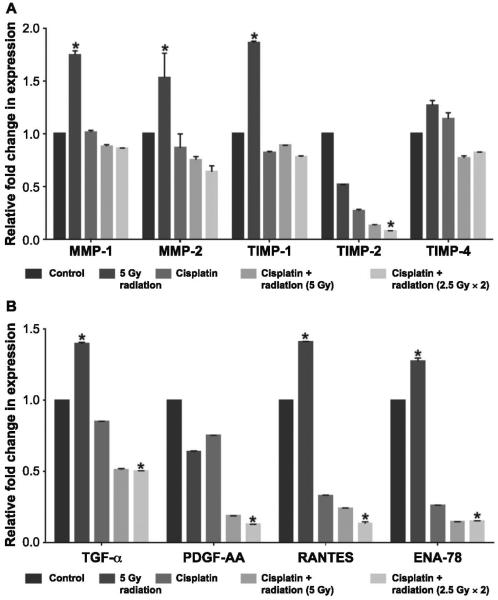
Lung cancer is the most common cause of cancer-related deaths worldwide and non-small cell lung cancer (NSCLC) accounts for ~85% of all lung cancer. While recent research has shown that cancer stem cells (CSC) exhibit radioresistant and chemoresistant properties, current cancer therapy targets the bulk of the tumor burden without accounting for the CSC and the contribution of the tumor microenvironment. CSC interaction with the stroma enhances NSCLC survival, thus limiting the efficacy of treatment. The aim of this study was to elucidate the role of CSC and the microenvironment in conferring radio- or chemoresistance in an in vitro tumor model for NSCLC. The novel in vitro three-dimensional (3D) NSCLC model of color-coded tumor tissue analogs (TTA) that we have developed is comprised of human lung adenocarcinoma cells, fibroblasts, endothelial cells and NSCLC cancer stem cells maintained in low oxygen conditions (5% O2) to recapitulate the physiologic conditions in tumors. Using this model, we demonstrate that a single 5 Gy radiation dose does not inhibit growth of TTA containing CSC and results in elevated expression of cytokines (TGF-α, RANTES, ENA-78) and factors (vimentin, MMP and TIMP), indicative of an invasive and aggressive phenotype. However, combined treatment of single dose or fractionated doses with cisplatin was found to either attenuate or decrease the proliferative effect that radiation exposure alone had on TTA containing CSC maintained in hypoxic conditions. In summary, we utilized a 3D NSCLC model, which had characteristics of the tumor microenvironment and tumor cell heterogeneity, to elucidate the multifactorial nature of radioresistance in tumors.
Figures

References
-
- Cancer Facts and Figures. American Cancer Society; 2015. bit.ly/1tMudoF.
-
- Price A. Emerging developments of chemoradiotherapy in stage III NSCLC. Nat Rev Clin Oncol. 2012;9:591–8. - PubMed
-
- Jett JR, Schild SE, Keith RL, Kesler KA, American College of Chest Physicians Treatment of non-small cell lung cancer, stage IIIB: ACCP evidence-based clinical practice guidelines (2nd edition) Chest. 2007;132:266S–76S. - PubMed
-
- Robinson LA, Ruckdeschel JC, Wagner H, Jr., Stevens CW, American College of Chest Physicians Treatment of non-small cell lung cancer-stage IIIA: ACCP evidence-based clinical practice guidelines (2nd edition) Chest. 2007;132:243S–65S. - PubMed
-
- Auperin A, Le Pechoux C, Rolland E, Curran WJ, Furuse K, Fournel P, et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J Clin Oncol. 2010;28:2181–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
