

Crises in Sickle Cell Disease
- PMID: 26836899
- PMCID: PMC6637264
- DOI: 10.1016/j.chest.2015.12.016
Crises in Sickle Cell Disease
Abstract
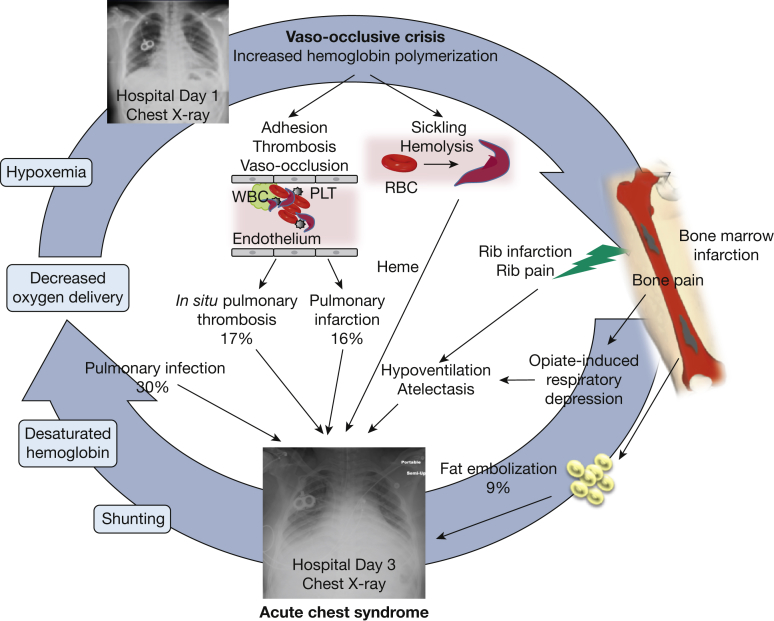
In spite of significant strides in the treatment of sickle cell disease (SCD), SCD crises are still responsible for high morbidity and early mortality. While most patients initially seek care in the acute setting for a seemingly uncomplicated pain episode (pain crisis or vaso-occlusive crisis), this initial event is the primary risk factor for potentially life-threatening complications. The pathophysiological basis of these illnesses is end-organ ischemia and infarction combined with the downstream effects of hemolysis that results from red blood cell sickling. These pathological changes can occur acutely and lead to a dramatic clinical presentation, but are frequently superimposed over a milieu of chronic vasculopathy, immune dysregulation, and decreased functional reserve. In the lungs, acute chest syndrome is a particularly ominous lung injury syndrome with a complex pathogenesis and potentially devastating sequelae, but all organ systems can be affected. It is, therefore, critical to understand the SCD patients' susceptibility to acute complications and their risk factors so that they can be recognized promptly and managed effectively. Blood transfusions remain the mainstay of therapy for all severe acute crises. Recommendations and indications for the safest and most efficient implementation of transfusion strategies in the critical care setting are therefore presented and discussed, together with their pitfalls and potential future therapeutic alternatives. In particular, the importance of extended phenotypic red blood cell matching cannot be overemphasized, due to the high prevalence of severe complications from red cell alloimmunization in SCD.
Keywords: acute chest syndrome; red blood cells; sickle cell disease; transfusion.
Copyright © 2016 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Akinola N.O., Stevens S.M., Franklin I.M. Rheological changes in the prodromal and established phases of sickle cell vaso-occlusive crisis. Br J Haematol. 1992;81(4):598–602. - PubMed
-
- Hebbel R.P. Blockade of adhesion of sickle cells to endothelium by monoclonal antibodies. N Engl J Med. 2000;342(25):1910–1912. - PubMed
-
- Hebbel R.P., Boogaerts M.A., Eaton J.W. Erythrocyte adherence to endothelium in sickle-cell anemia: a possible determinant of disease severity. N Engl J Med. 1980;302(18):992–995. - PubMed
-
- Hebbel R.P., Boogaerts M.A., Koresawa S. Erythrocyte adherence to endothelium as a determinant of vasocclusive severity in sickle cell disease. Trans Assoc Am Physicians. 1980;93:94–99. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
