

Pleural Effusions at First ED Encounter Predict Worse Clinical Outcomes in Patients With Pneumonia
- PMID: 26836918
- PMCID: PMC6026265
- DOI: 10.1016/j.chest.2015.12.027
Pleural Effusions at First ED Encounter Predict Worse Clinical Outcomes in Patients With Pneumonia
Abstract
Background: Pleural effusions are present in 15% to 44% of hospitalized patients with pneumonia. It is unknown whether effusions at first presentation to the ED influence outcomes or should be managed differently.
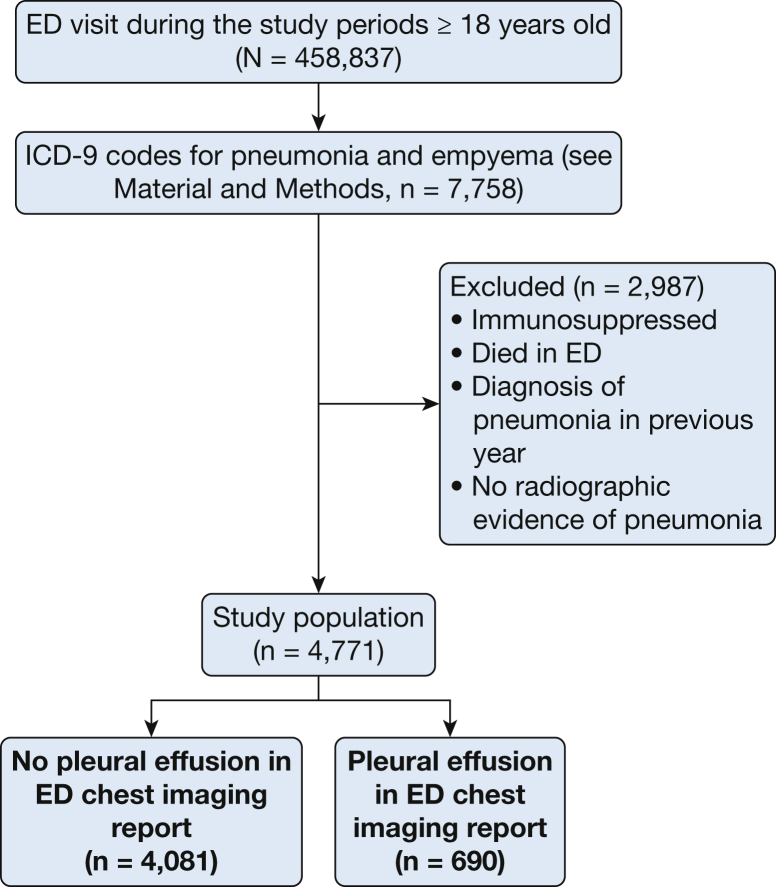
Methods: We studied patients in seven hospital EDs with International Statistical Classification of Disease and Health Related Problems-Version 9 codes for pneumonia, or empyema, sepsis, or respiratory failure with secondary pneumonia. Patients with no confirmatory findings on chest imaging were excluded. Pleural effusions were identified with the use of radiographic imaging.
Results: Over 24 months, 4,771 of 458,837 adult ED patients fulfilled entry criteria. Among the 690 (14.5%) patients with pleural effusions, their median age was 68 years, and 46% were male. Patients with higher Elixhauser comorbidity scores (OR, 1.13 [95% CI, 1.09-1.18]; P < .001), brain natriuretic peptide levels (OR, 1.20 [95% CI, 1.12-1.28]; P < .001), bilirubin levels (OR, 1.07 [95% CI, 1.00-1.15]; P = .04), and age (OR, 1.15 [95% CI, 1.09-1.21]; P < .001) were more likely to have parapneumonic effusions. In patients without effusion, electronic version of CURB-65 (confusion, uremia, respiratory rate, BP, age ≥ 65 years accurately predicted mortality (4.7% predicted vs 5.0% actual). However, eCURB underestimated mortality in those with effusions (predicted 7.0% vs actual 14.0%; P < .001). Patients with effusions were more likely to be admitted (77% vs 57%; P < .001) and had a longer hospital stay (median, 2.8 vs 1.3 days; P < .001). After severity adjustment, the likelihood of 30-day mortality was greater among patients with effusions (OR, 2.6 [CI, 2.0-3.5]; P < .001), and hospital stay was disproportionately longer (coefficient, 0.22 [CI, 0.14-0.29]; P < .001).
Conclusions: Patients with pneumonia and pleural effusions at ED presentation in this study were more likely to die, be admitted, and had longer hospital stays. Why parapneumonic effusions are associated with adverse outcomes, and whether different management of these patients might improve outcome, needs urgent investigation.
Keywords: brain natriuretic peptide; emergency medicine; pleural effusion; pneumonia.
Copyright © 2016 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Center for Health Statistics. Health, United States, May 20, 2010. Centers for Disease Control and Prevention website. http://www.cdc.gov/nchs/data/nvsr58/nvsr58_19.pdf. Accessed January 9, 2015.
-
- Marston B.J., Plouffe J.F., File T.M., Jr., the Community-Based Pneumonia Incidence Study Group Incidence of community-acquired pneumonia requiring hospitalization. Results of a population-based active surveillance study in Ohio. Arch Intern Med. 1997;157(15):1709–1718. - PubMed
-
- Niederman M.S., McCombs J.S., Unger A.N., Kumar A., Popovian R. The cost of treating community-acquired pneumonia. Clin Ther. 1998;20(4):820–837. - PubMed
-
- Falguera M., Carratala J., Bielsa S. Predictive factors, microbiology, and outcome of patients with parapneumonic effusion. Eur Resp J. 2011;38(5):1173–1179. - PubMed
-
- Skouras V., Awdankiewicz A., Light R.W. What size parapneumonic effusions should be sampled? Thorax. 2010;65(1):91. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
