

Risk of Injurious Fall and Hip Fracture up to 26 y before the Diagnosis of Parkinson Disease: Nested Case-Control Studies in a Nationwide Cohort
- PMID: 26836965
- PMCID: PMC4737490
- DOI: 10.1371/journal.pmed.1001954
Risk of Injurious Fall and Hip Fracture up to 26 y before the Diagnosis of Parkinson Disease: Nested Case-Control Studies in a Nationwide Cohort
Abstract
Background: Low muscle strength has been found in late adolescence in individuals diagnosed with Parkinson disease (PD) 30 y later. This study investigated whether this lower muscle strength also may translate into increased risks of falling and fracture before the diagnosis of PD.
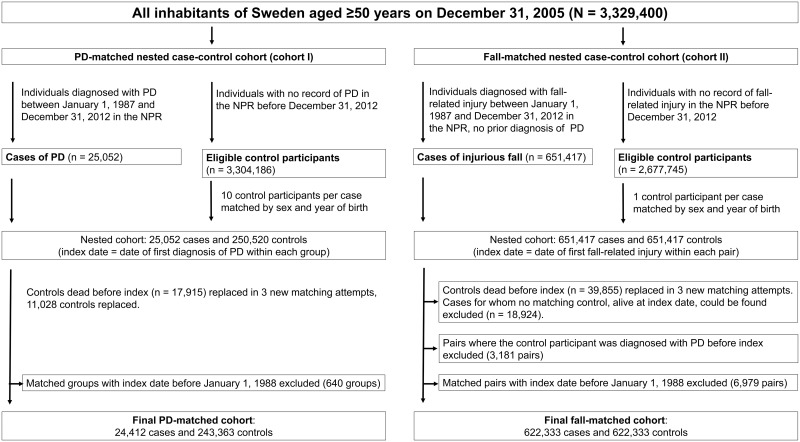
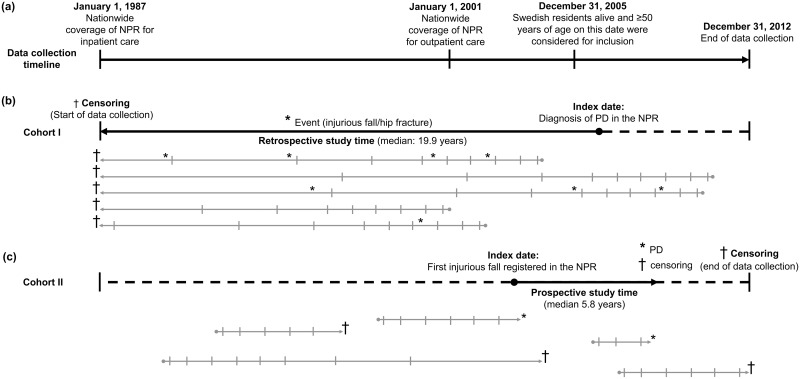
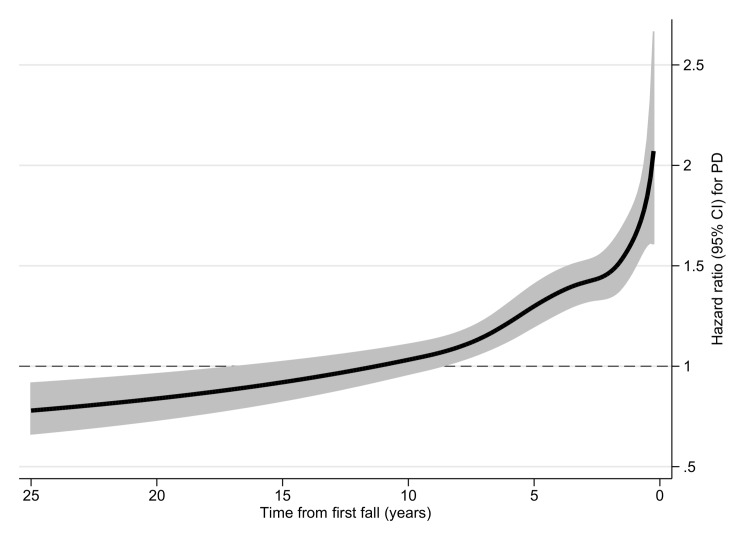
Methods and findings: Among all Swedish citizens aged ≥50 y in 2005, two nested case-control cohorts were compiled. In cohort I, individuals diagnosed with PD during 1988-2012 (n = 24,412) were matched with up to ten controls (n = 243,363), and the risk of fall-related injuries before diagnosis of PD was evaluated. In cohort II, individuals with an injurious fall in need of emergency care during 1988-2012 (n = 622,333) were matched with one control (n = 622,333), and the risk of PD after the injurious fall was evaluated. In cohort I, 18.0% of cases and 11.5% of controls had at least one injurious fall (p < 0.001) prior to PD diagnosis in the case. Assessed by conditional logistic regression analysis adjusted for comorbid diagnoses and education level, PD was associated with increased risks of injurious fall up to 10 y before diagnosis (odds ratio [OR] 1.19, 95% CI 1.08-1.31; 7 to <10 y before diagnosis) and hip fracture ≥15 y before diagnosis (OR 1.36, 95% CI 1.10-1.69; 15-26 y before diagnosis). In cohort II, 0.7% of individuals with an injurious fall and 0.5% of controls were diagnosed with PD during follow-up (p < 0.001). The risk of PD was increased for up to 10 y after an injurious fall (OR 1.18, 95% CI 1.02-1.37; 7 to <10 y after diagnosis). An important limitation is that the diagnoses were obtained from registers and could not be clinically confirmed for the study.
Conclusions: The increased risks of falling and hip fracture prior to the diagnosis of PD may suggest the presence of clinically relevant neurodegenerative impairment many years before the diagnosis of this disease.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Comment in
-
Parkinson's disease diagnosis is preceded by increased risk of falls, study finds.BMJ. 2016 Feb 4;352:i695. doi: 10.1136/bmj.i695. BMJ. 2016. PMID: 26849893 No abstract available.
References
-
- Grimbergen YA, Munneke M, Bloem BR. Falls in Parkinson’s disease. Curr Opin Neurol. 2004;17:405–415. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
