

Trends in Follow-Up of Patients Presenting to the Emergency Department with Symptomatic Cholelithiasis
- PMID: 26837281
- PMCID: PMC4818112
- DOI: 10.1016/j.jamcollsurg.2015.12.011
Trends in Follow-Up of Patients Presenting to the Emergency Department with Symptomatic Cholelithiasis
Abstract
Background: Fewer than 25% of Medicare beneficiaries presenting with symptomatic cholelithiasis undergo elective cholecystectomy. To better understand underuse of cholecystectomy, we examined physician follow-up patterns after emergency department (ED) visits for symptomatic gallstones.
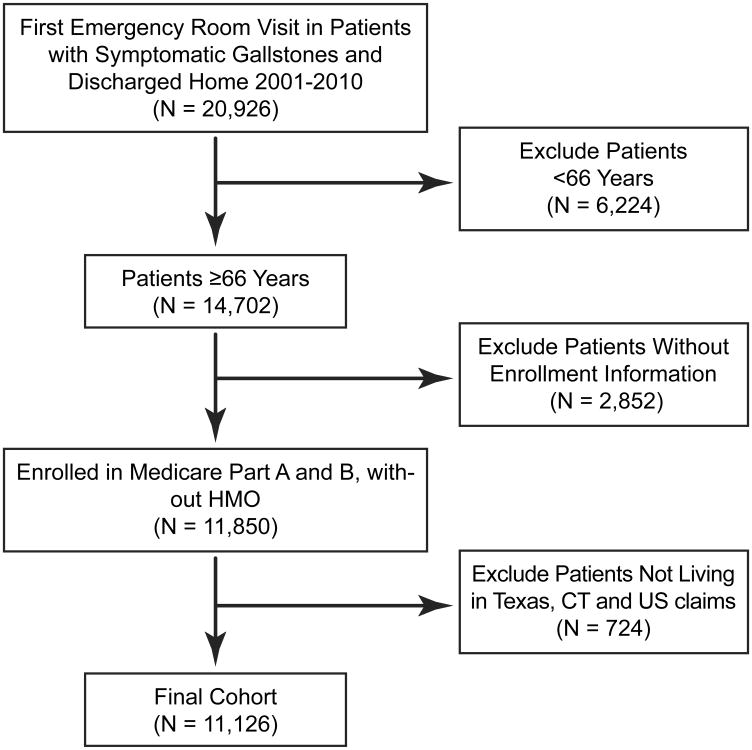
Study design: We used 100% Texas Medicare claims (2001 to 2010) to identify patients 66 years of age and older who presented to the ED with symptomatic cholelithiasis and were discharged home without cholecystectomy. Timing of outpatient physician visits after ED discharge and rates of emergent cholecystectomy based on physician follow-up patterns were compared.
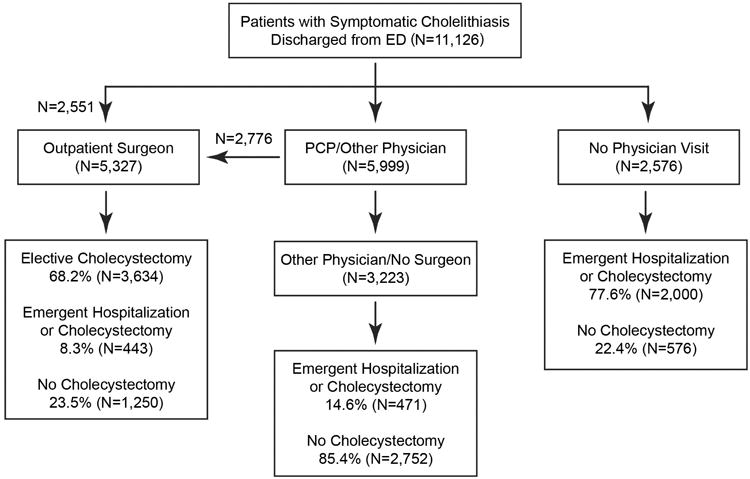
Results: In total, 11,126 patients presented to the ED with symptomatic cholelithiasis and were discharged without cholecystectomy. After discharge, 5,327 patients (47.9%) had an outpatient surgeon visit, 29.0% saw another physician and never saw a surgeon, and 23.1% never saw a physician; 68.2% of patients who saw a surgeon underwent elective cholecystectomy; and 8.3% of patients who saw a surgeon, 14.6% of patients who saw other physicians and no surgeon, and 77.6% of patients who never saw any physician, required emergent hospitalization (p < 0.0001). For people who did not see a physician, mean time to emergent hospitalization was 7.5 days (median 2 days); 95.9% presented within 2 weeks after their initial presentation.
Conclusions: Fewer than half of patients were evaluated by a surgeon after an initial ED visit for symptomatic gallstones. Patients who did not have physician follow-up were most likely to require emergent cholecystectomy, suggesting inappropriate ED discharge and highlighting the need for timely follow-up. Early outpatient surgical consultation is critical in determining appropriateness for cholecystectomy and avoiding emergent cholecystectomy in older patients with symptomatic gallstones.
Copyright © 2016 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Discussion.J Am Coll Surg. 2016 Apr;222(4):385-6. doi: 10.1016/j.jamcollsurg.2016.01.042. J Am Coll Surg. 2016. PMID: 27016965 No abstract available.
Similar articles
-
Hospital readmission after emergency room visit for cholelithiasis.J Surg Res. 2015 Aug;197(2):318-23. doi: 10.1016/j.jss.2015.04.032. Epub 2015 Apr 16. J Surg Res. 2015. PMID: 25959838 Free PMC article.
-
The risk paradox: use of elective cholecystectomy in older patients is independent of their risk of developing complications.J Am Coll Surg. 2015 Apr;220(4):682-90. doi: 10.1016/j.jamcollsurg.2014.12.012. Epub 2014 Dec 17. J Am Coll Surg. 2015. PMID: 25660731 Free PMC article.
-
PREOP-Gallstones: A Prognostic Nomogram for the Management of Symptomatic Cholelithiasis in Older Patients.Ann Surg. 2015 Jun;261(6):1184-90. doi: 10.1097/SLA.0000000000000868. Ann Surg. 2015. PMID: 25072449 Free PMC article.
-
Natural history of asymptomatic and symptomatic gallstones.Am J Surg. 1993 Apr;165(4):399-404. doi: 10.1016/s0002-9610(05)80930-4. Am J Surg. 1993. PMID: 8480871 Review.
-
Management of symptomatic cholelithiasis: a systematic review.Syst Rev. 2022 Dec 12;11(1):267. doi: 10.1186/s13643-022-02135-8. Syst Rev. 2022. PMID: 36510302 Free PMC article.
Cited by
-
Decreased Emergency Cholecystectomy and Case Fatality Rate, Not Explained by Expansion of Medicaid.J Surg Res. 2023 Aug;288:350-361. doi: 10.1016/j.jss.2023.03.006. Epub 2023 Apr 14. J Surg Res. 2023. PMID: 37060861 Free PMC article.
-
How Safe is Performing Cholecystectomy in the Oldest Old? A 15-year Retrospective Study from a Single Institution.World J Surg. 2018 Jan;42(1):73-81. doi: 10.1007/s00268-017-4147-8. World J Surg. 2018. PMID: 28741196
References
-
- Bergman S, Sourial N, Vedel I, et al. Gallstone disease in the elderly: are older patients managed differently? Surg Endosc. 2011 Jan;25(1):55–61. - PubMed
-
- Lirussi F, Nassuato G, Passera D, et al. Gallstone disease in an elderly population: the Silea study. Eur J Gastroenterol Hepatol. 1999 May;11(5):485–491. - PubMed
-
- Ratner J, Lisbona A, Rosenbloom M, Palayew M, Szabolcsi S, Tupaz T. The prevalence of gallstone disease in very old institutionalized persons. Jama. 1991 Feb 20;265(7):902–903. - PubMed
-
- Overby DW, Apelgren KN, Richardson W, Fanelli R Society of American G, Endoscopic S. SAGES guidelines for the clinical application of laparoscopic biliary tract surgery. Surg Endosc. 2010 Oct;24(10):2368–2386. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
