

Benzodiazepine use and risk of incident dementia or cognitive decline: prospective population based study
- PMID: 26837813
- PMCID: PMC4737849
- DOI: 10.1136/bmj.i90
Benzodiazepine use and risk of incident dementia or cognitive decline: prospective population based study
Abstract
Objective: To determine whether higher cumulative use of benzodiazepines is associated with a higher risk of dementia or more rapid cognitive decline.
Design: Prospective population based cohort.
Setting: Integrated healthcare delivery system, Seattle, Washington.
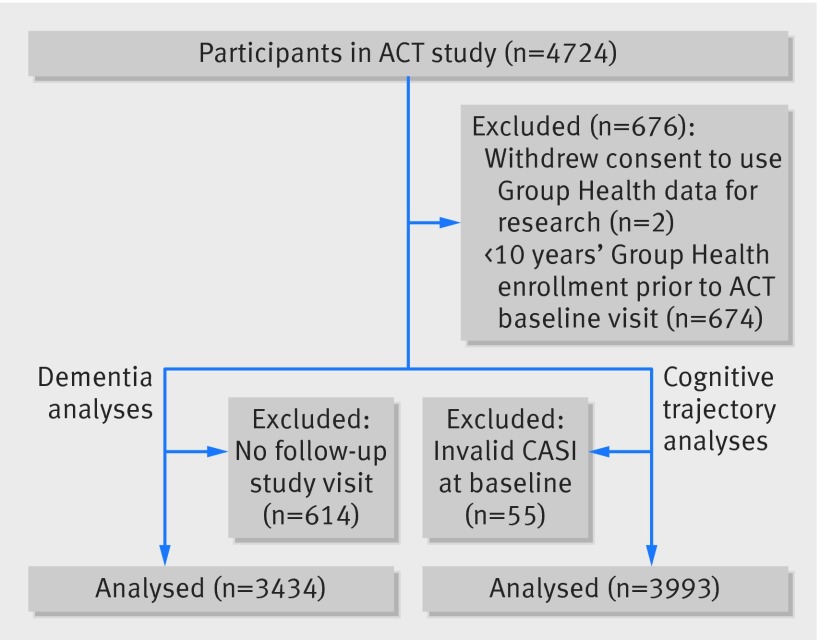
Participants: 3434 participants aged ≥ 65 without dementia at study entry. There were two rounds of recruitment (1994-96 and 2000-03) followed by continuous enrollment beginning in 2004.
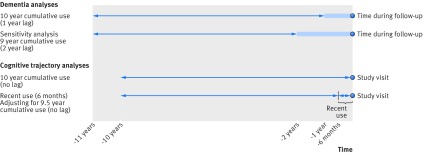
Main outcomes measures: The cognitive abilities screening instrument (CASI) was administered every two years to screen for dementia and was used to examine cognitive trajectory. Incident dementia and Alzheimer's disease were determined with standard diagnostic criteria. Benzodiazepine exposure was defined from computerized pharmacy data and consisted of the total standardized daily doses (TSDDs) dispensed over a 10 year period (a rolling window that moved forward in time during follow-up). The most recent year was excluded because of possible use for prodromal symptoms. Multivariable Cox proportional hazard models were used to examine time varying use of benzodiazepine and dementia risk. Analyses of cognitive trajectory used linear regression models with generalized estimating equations.
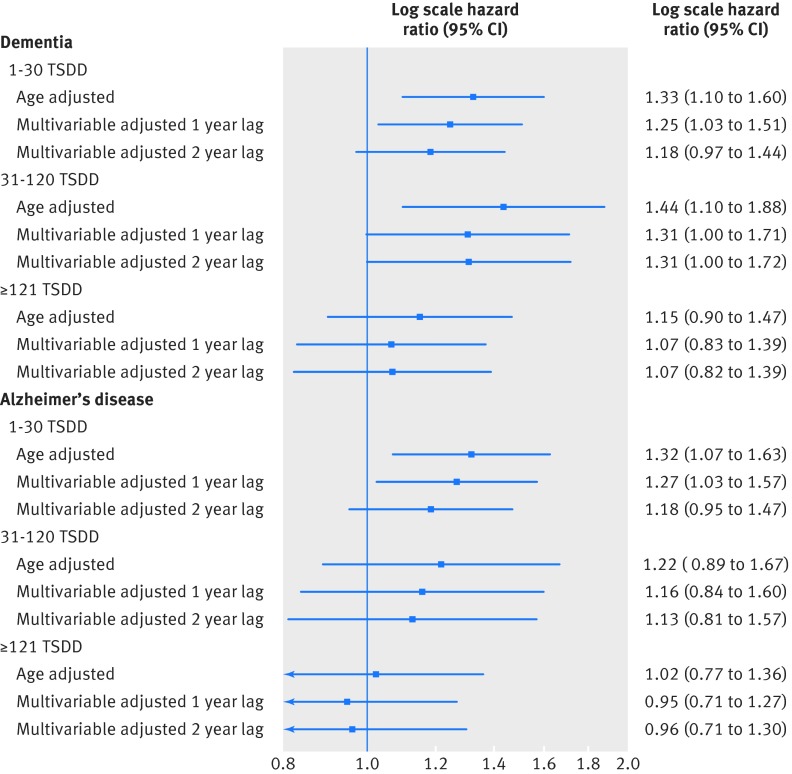
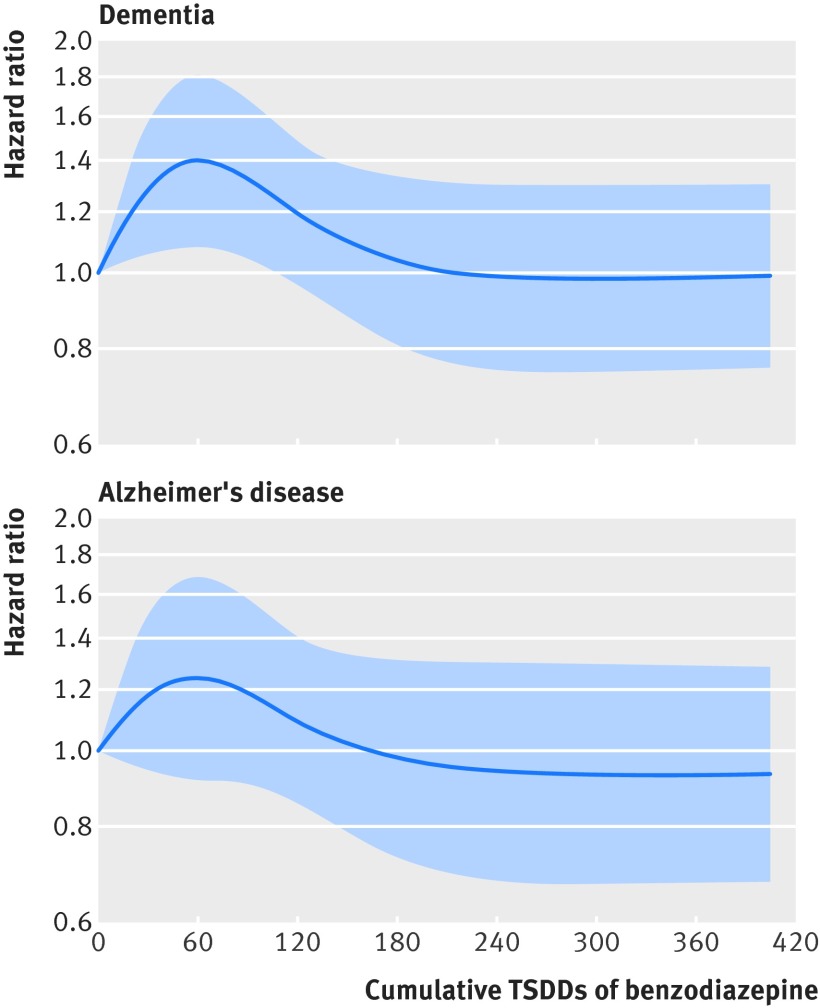
Results: Over a mean follow-up of 7.3 years, 797 participants (23.2%) developed dementia, of whom 637 developed Alzheimer's disease. For dementia, the adjusted hazard ratios associated with cumulative benzodiazepine use compared with non-use were 1.25 (95% confidence interval 1.03 to 1.51) for 1-30 TSDDs; 1.31 (1.00 to 1.71) for 31-120 TSDDs; and 1.07 (0.82 to 1.39) for ≥ 121 TSDDs. Results were similar for Alzheimer's disease. Higher benzodiazepine use was not associated with more rapid cognitive decline.
Conclusion: The risk of dementia is slightly higher in people with minimal exposure to benzodiazepines but not with the highest level of exposure. These results do not support a causal association between benzodiazepine use and dementia.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Similar articles
-
Prescription Opioids and Risk of Dementia or Cognitive Decline: A Prospective Cohort Study.J Am Geriatr Soc. 2015 Aug;63(8):1519-26. doi: 10.1111/jgs.13562. J Am Geriatr Soc. 2015. PMID: 26289681 Free PMC article. Clinical Trial.
-
Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study.JAMA Intern Med. 2015 Mar;175(3):401-7. doi: 10.1001/jamainternmed.2014.7663. JAMA Intern Med. 2015. PMID: 25621434 Free PMC article.
-
Cumulative Antidepressant Use and Risk of Dementia in a Prospective Cohort Study.J Am Geriatr Soc. 2018 Oct;66(10):1948-1955. doi: 10.1111/jgs.15508. Epub 2018 Sep 17. J Am Geriatr Soc. 2018. PMID: 30221747
-
Benzodiazepine use and cognitive decline in the elderly.Am J Health Syst Pharm. 2018 Jan 1;75(1):e6-e12. doi: 10.2146/ajhp160381. Am J Health Syst Pharm. 2018. PMID: 29273607 Review.
-
Is benzodiazepine use a risk factor for cognitive decline and dementia? A literature review of epidemiological studies.Psychol Med. 2005 Mar;35(3):307-15. doi: 10.1017/s0033291704003897. Psychol Med. 2005. PMID: 15841867 Review.
Cited by
-
Associations of benzodiazepine use with cognitive ability and age-related cognitive decline.Psychol Med. 2024 Oct 14;54(13):1-8. doi: 10.1017/S0033291724002046. Online ahead of print. Psychol Med. 2024. PMID: 39397686 Free PMC article.
-
Preoperative mild cognitive impairment as a risk factor of postoperative cognitive dysfunction in elderly patients undergoing spine surgery.Front Aging Neurosci. 2024 Jan 12;16:1292942. doi: 10.3389/fnagi.2024.1292942. eCollection 2024. Front Aging Neurosci. 2024. PMID: 38282693 Free PMC article.
-
Benzodiazepine use and the risk of dementia.Alzheimers Dement (N Y). 2022 Jul 20;8(1):e12309. doi: 10.1002/trc2.12309. eCollection 2022. Alzheimers Dement (N Y). 2022. PMID: 35874428 Free PMC article.
-
A Systematic Review and Meta-Analysis of the Risk of Dementia Associated with Benzodiazepine Use, After Controlling for Protopathic Bias.CNS Drugs. 2018 Jun;32(6):485-497. doi: 10.1007/s40263-018-0535-3. CNS Drugs. 2018. PMID: 29926372
-
Risk Factors for the Progression of Mild Cognitive Impairment in Different Types of Neurodegenerative Disorders.Behav Neurol. 2018 Jun 5;2018:6929732. doi: 10.1155/2018/6929732. eCollection 2018. Behav Neurol. 2018. PMID: 29971138 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical