

Impact of Cell Therapy on Myocardial Perfusion and Cardiovascular Outcomes in Patients With Angina Refractory to Medical Therapy: A Systematic Review and Meta-Analysis
- PMID: 26838794
- PMCID: PMC4798914
- DOI: 10.1161/CIRCRESAHA.115.308056
Impact of Cell Therapy on Myocardial Perfusion and Cardiovascular Outcomes in Patients With Angina Refractory to Medical Therapy: A Systematic Review and Meta-Analysis
Abstract
Rationale: The effect of stem/progenitor cells on myocardial perfusion and clinical outcomes in patients with refractory angina remains unclear because studies published to date have been small phase I-II trials.
Objective: We performed a meta-analysis of randomized controlled trials to evaluate the effect of cell-based therapy in patients with refractory angina who were ineligible for coronary revascularization.
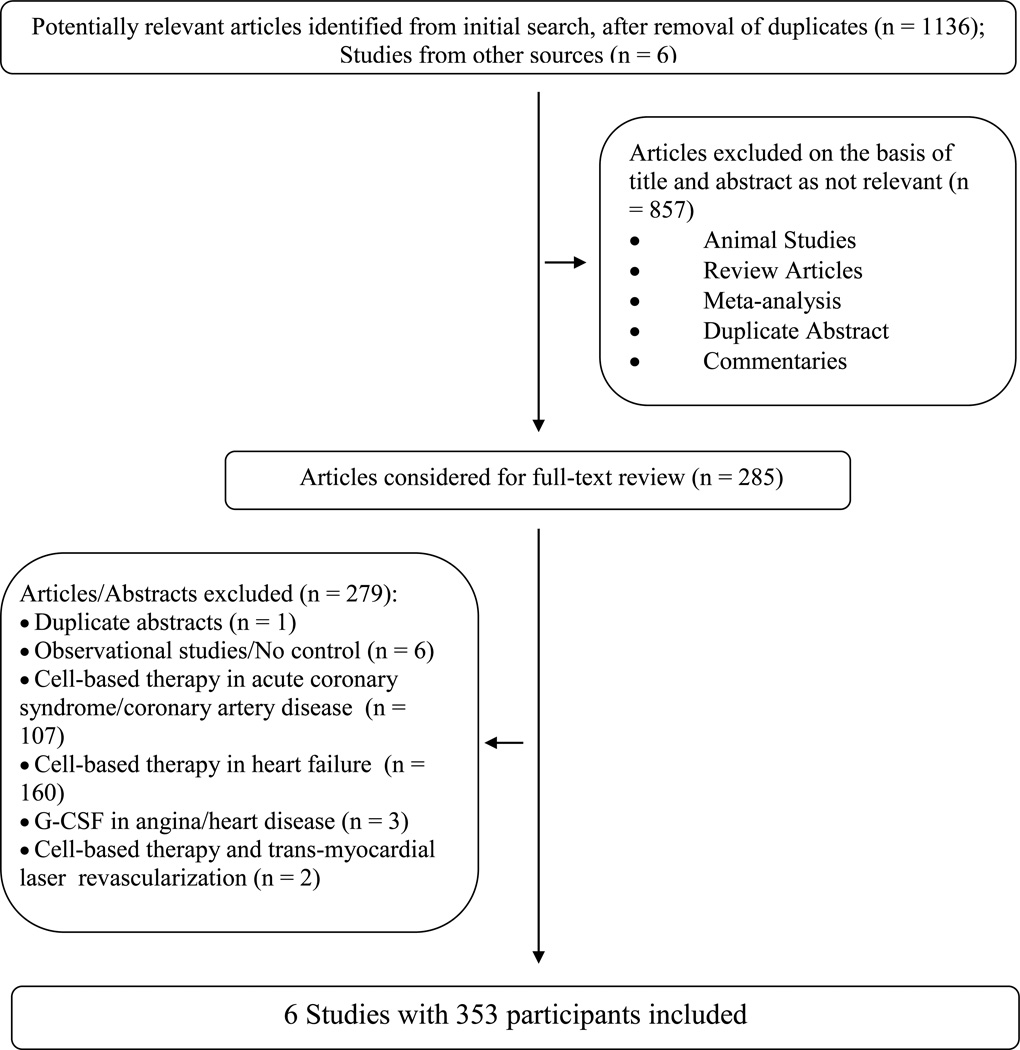
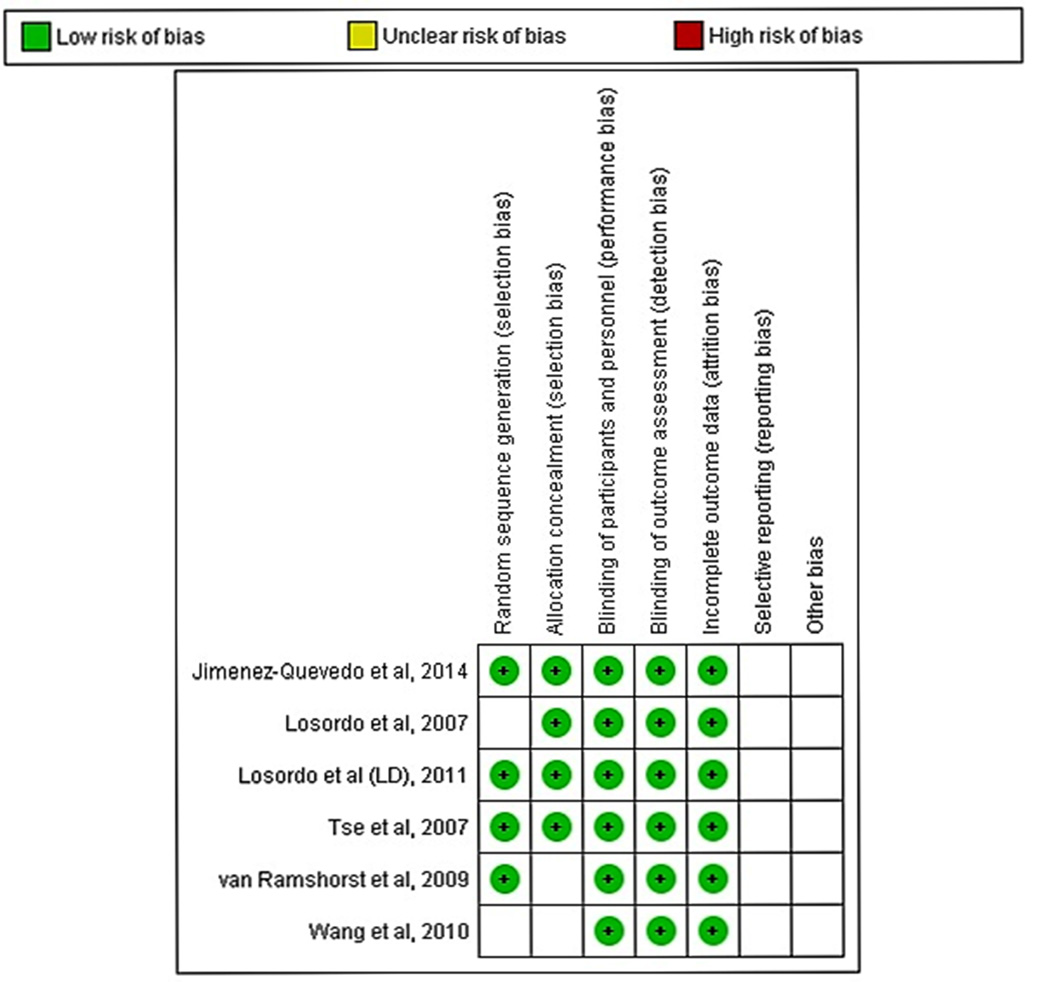
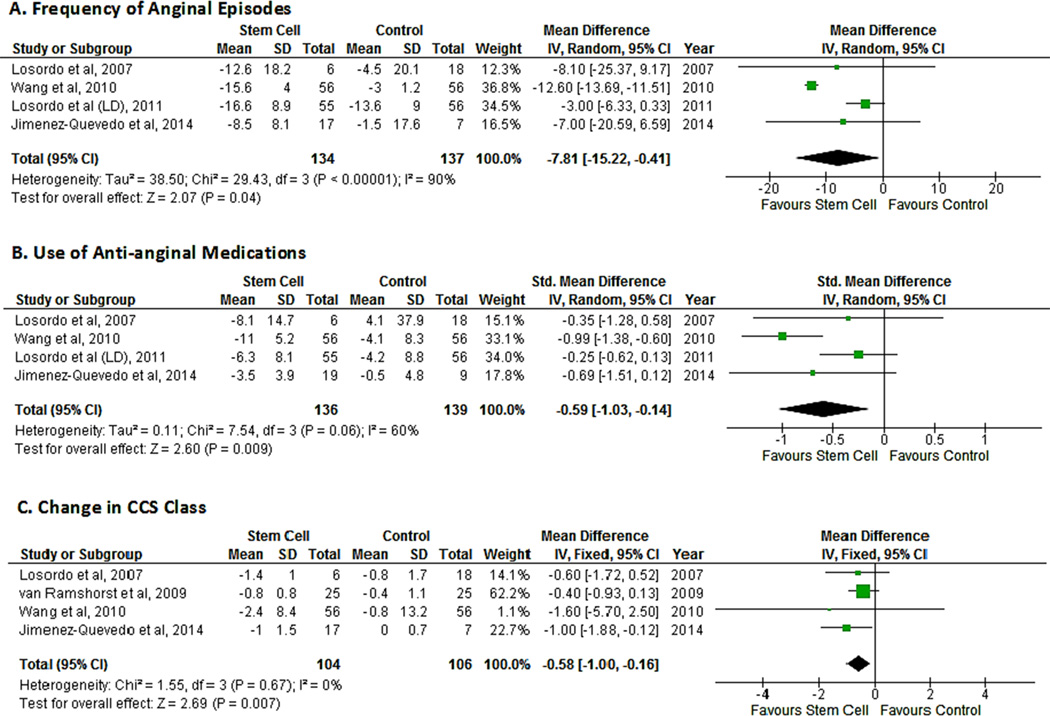
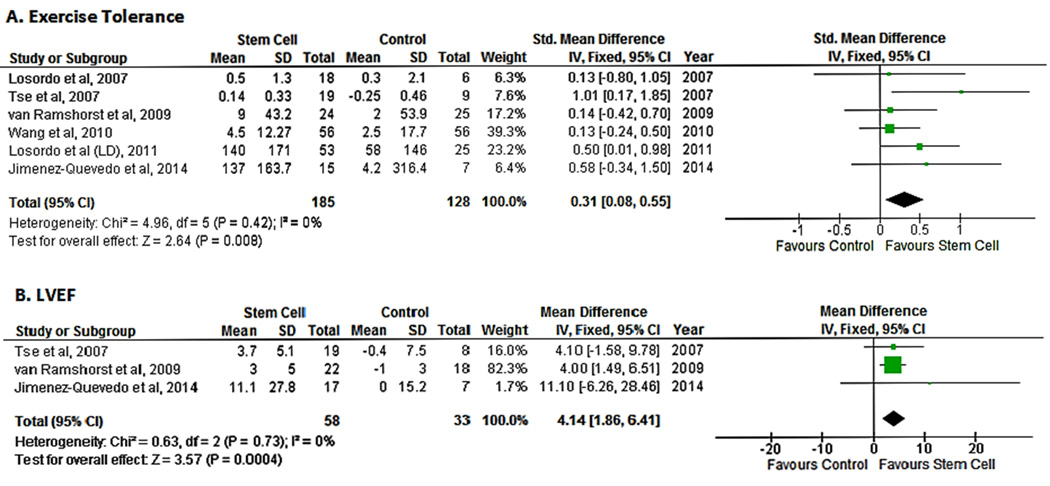
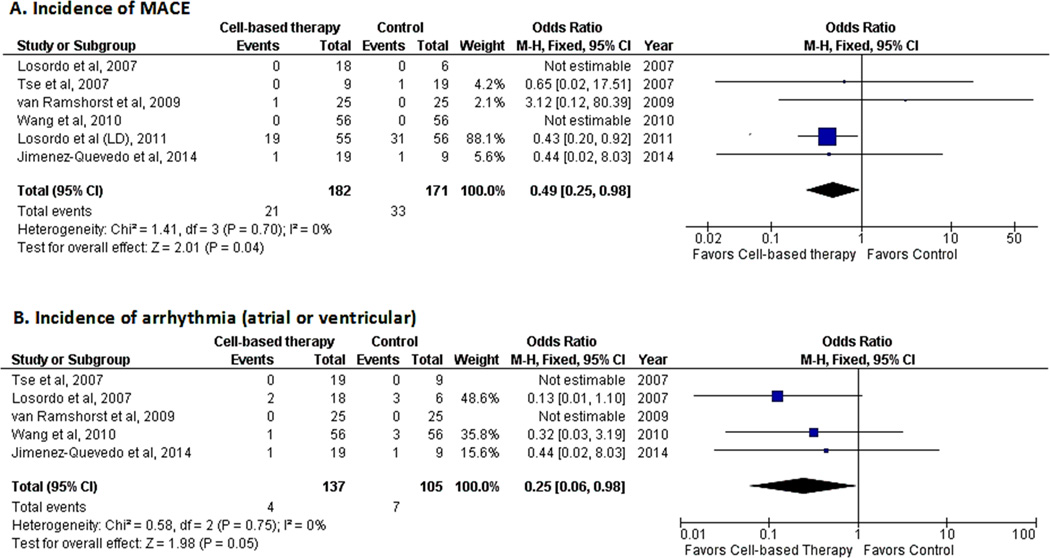
Methods and results: Several data sources were searched from inception to September 2015, which yielded 6 studies. The outcomes pooled were indices of angina (anginal episodes, Canadian Cardiovascular Society angina class, exercise tolerance, and antianginal medications), myocardial perfusion, and clinical end points. We combined the reported clinical outcomes (myocardial infarction, cardiac-related hospitalization, and mortality) into a composite end point (major adverse cardiac events). Mean difference (MD), standardized mean differences, or odds ratio were calculated to assess relevant outcomes. Our analysis shows an improvement in anginal episodes (MD, -7.81; 95% confidence interval [CI], -15.22 to -0.41), use of antianginal medications (standardized MD, -0.59; 95% CI, -1.03 to -0.14), Canadian Cardiovascular Society class (MD, -0.58; 95% CI, -1.00 to -0.16), exercise tolerance (standardized MD, 0.331; 95% CI, 0.08 to 0.55), and myocardial perfusion (standardized MD, -0.49; 95% CI, -0.76 to -0.21) and a decreased risk of major adverse cardiac events (odds ratio, 0.49; 95% CI, 0.25 to 0.98) and arrhythmias (odds ratio, 0.25; 95% CI, 0.06 to 0.98) in cell-treated patients when compared with patients on maximal medical therapy.
Conclusions: The present meta-analysis indicates that cell-based therapies are not only safe but also lead to an improvement in indices of angina, relevant clinical outcomes, and myocardial perfusion in patients with refractory angina. These encouraging results suggest that larger, phase III randomized controlled trials are in order to conclusively determine the effect of stem/progenitor cells in refractory angina.
Keywords: cell- and tissue-based therapy; meta-analysis; perfusion; randomized controlled trial; stem cells.
© 2016 American Heart Association, Inc.
Figures

Comment in
-
Cell Therapy Augments Myocardial Perfusion and Improves Quality of Life in Patients With Refractory Angina.Circ Res. 2016 Mar 18;118(6):911-5. doi: 10.1161/CIRCRESAHA.116.308409. Circ Res. 2016. PMID: 26987911 Free PMC article. No abstract available.
References
-
- McGillion M, Arthur HM, Cook A, Carroll SL, Victor JC, L'Allier PL, Jolicoeur EM, Svorkdal N, Niznick J, Teoh K, Cosman T, Sessle B, Watt-Watson J, Clark A, Taenzer P, Coyte P, Malysh L, Galte C, Stone J Canadian Cardiovascular S, Canadian Pain S. Management of patients with refractory angina: Canadian cardiovascular society/canadian pain society joint guidelines. The Canadian journal of cardiology. 2012;28:S20–S41. - PubMed
-
- Mukherjee D, Bhatt DL, Roe MT, Patel V, Ellis SG. Direct myocardial revascularization and angiogenesis--how many patients might be eligible? The American journal of cardiology. 1999;84:598–600. A598. - PubMed
-
- Henry TD, Satran D, Jolicoeur EM. Treatment of refractory angina in patients not suitable for revascularization. Nature reviews. Cardiology. 2014;11:78–95. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
