

Errors in imaging patients in the emergency setting
- PMID: 26838955
- PMCID: PMC4985468
- DOI: 10.1259/bjr.20150914
Errors in imaging patients in the emergency setting
Abstract
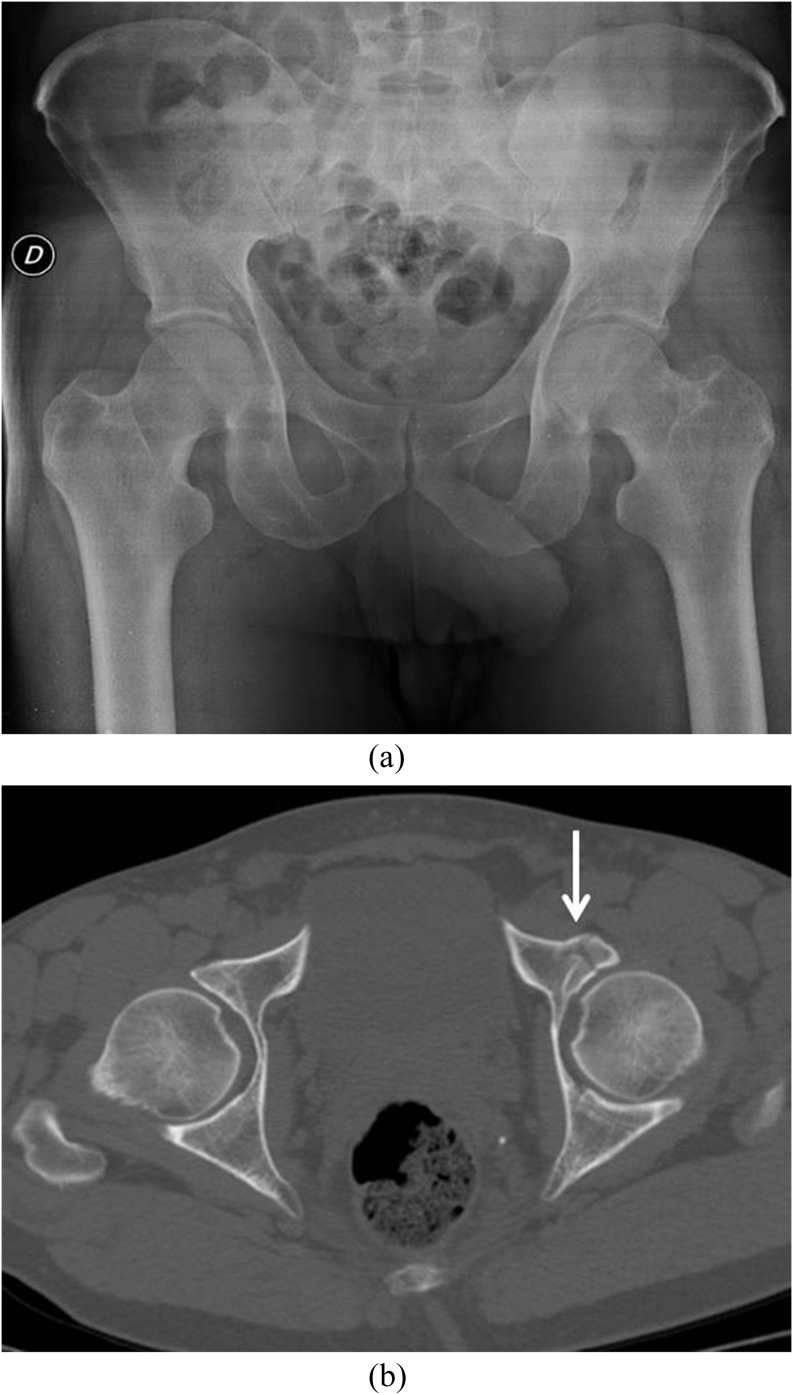
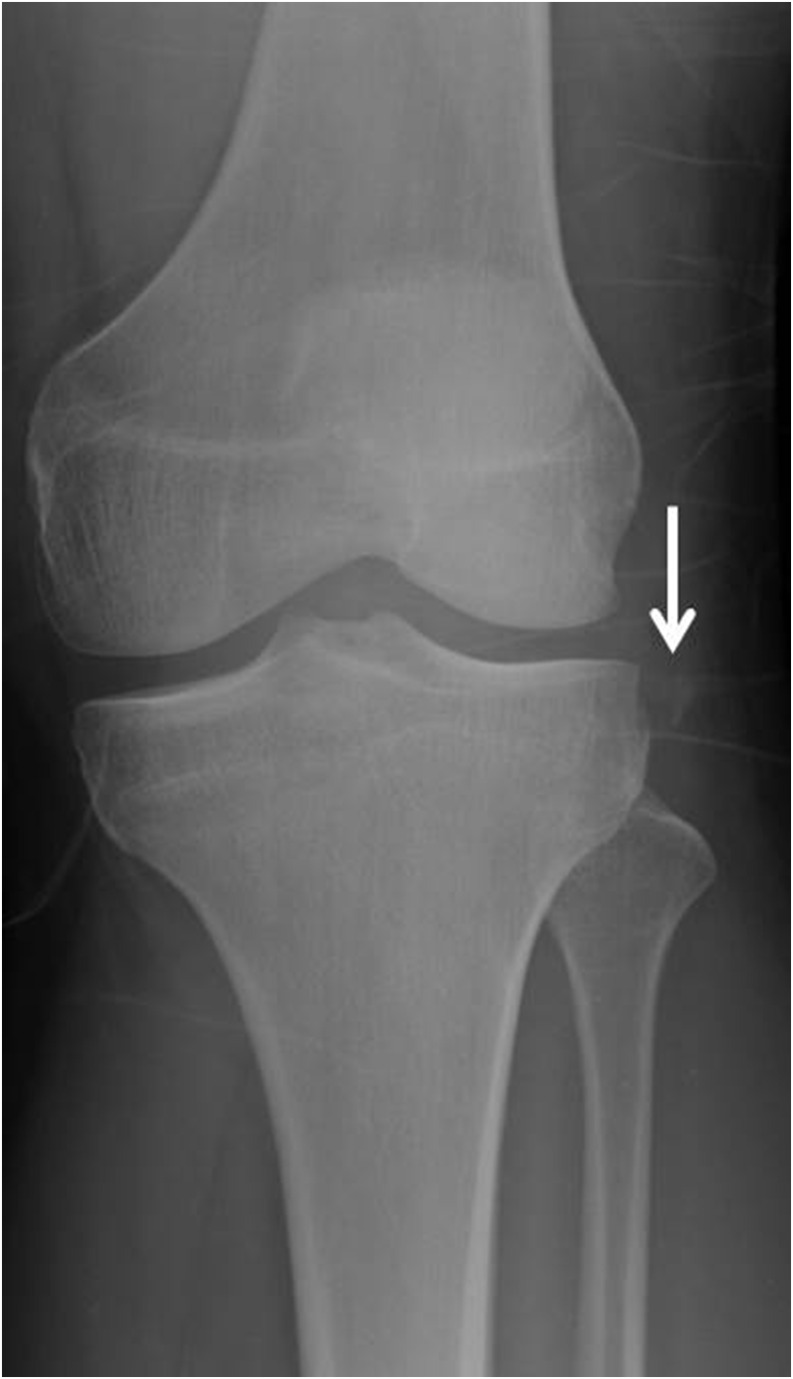
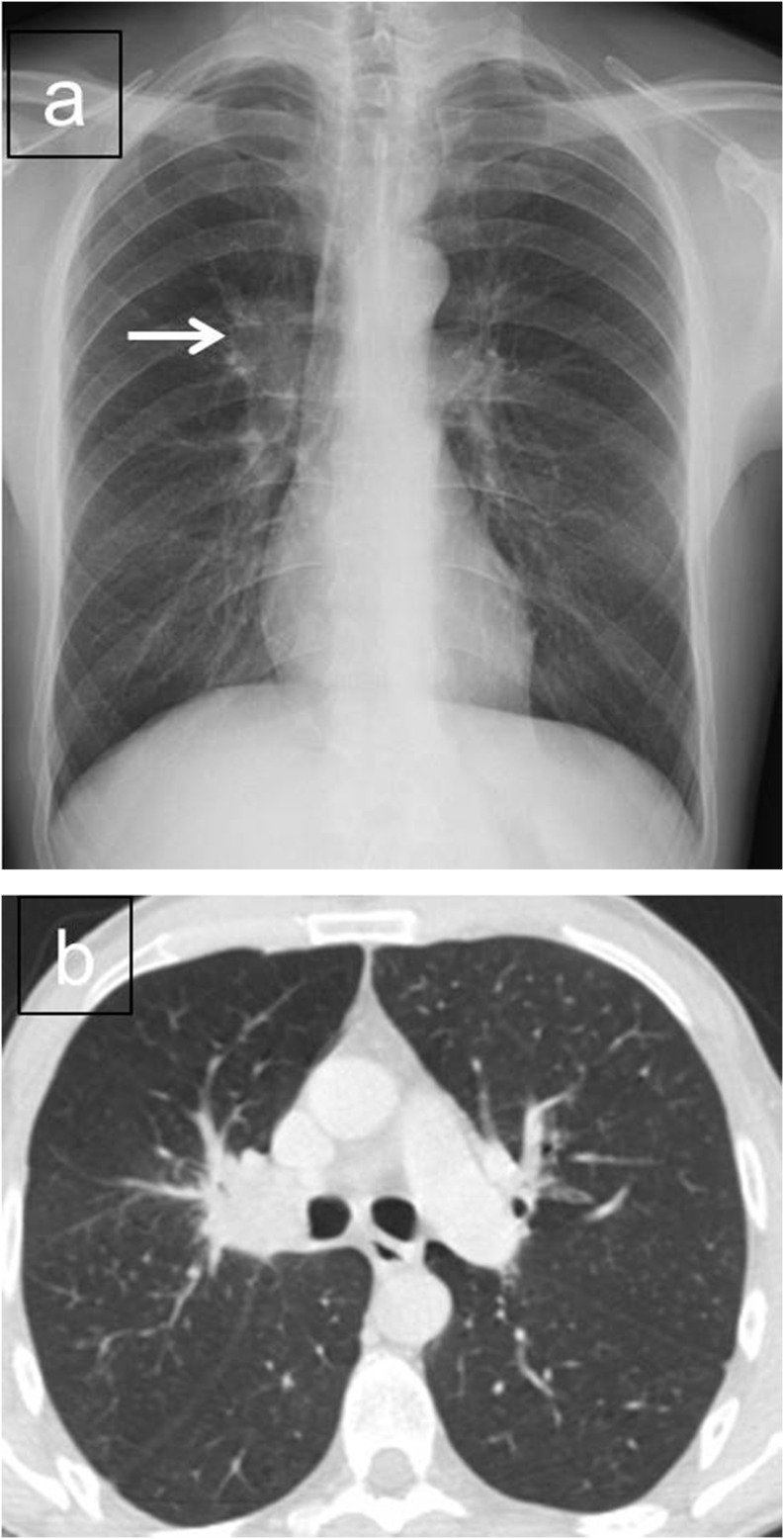
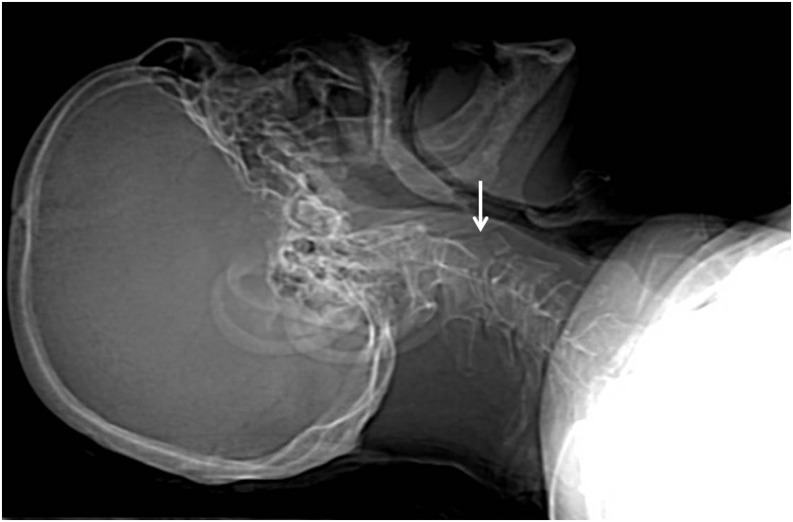
Emergency and trauma care produces a "perfect storm" for radiological errors: uncooperative patients, inadequate histories, time-critical decisions, concurrent tasks and often junior personnel working after hours in busy emergency departments. The main cause of diagnostic errors in the emergency department is the failure to correctly interpret radiographs, and the majority of diagnoses missed on radiographs are fractures. Missed diagnoses potentially have important consequences for patients, clinicians and radiologists. Radiologists play a pivotal role in the diagnostic assessment of polytrauma patients and of patients with non-traumatic craniothoracoabdominal emergencies, and key elements to reduce errors in the emergency setting are knowledge, experience and the correct application of imaging protocols. This article aims to highlight the definition and classification of errors in radiology, the causes of errors in emergency radiology and the spectrum of diagnostic errors in radiography, ultrasonography and CT in the emergency setting.
Figures



References
-
- West RW. Radiology malpractice in the emergency room setting. Emerg Radiol 2000; 7: 14–18. doi: 10.1007/s101400050004 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
