

Racial Differences in Outcomes of an Advance Care Planning Intervention for Dialysis Patients and Their Surrogates
- PMID: 26840848
- PMCID: PMC4753624
- DOI: 10.1089/jpm.2015.0232
Racial Differences in Outcomes of an Advance Care Planning Intervention for Dialysis Patients and Their Surrogates
Abstract
Background: African Americans' beliefs about end-of-life care may differ from those of whites, but racial differences in advance care planning (ACP) outcomes are unknown.
Objective: The aim of this study was to compare the efficacy of an ACP intervention on preparation for end-of-life decision making and post-bereavement outcomes for African Americans and whites on dialysis.
Method: A secondary analysis of data from a randomized trial comparing an ACP intervention (Sharing Patient's Illness Representations to Increase Trust [SPIRIT]) with usual care was conducted. There were 420 participants, 210 patient-surrogate dyads (67.4% African Americans), recruited from 20 dialysis centers in North Carolina. The outcomes of preparation for end-of-life decision making included dyad congruence on goals of care, surrogate decision-making confidence, a composite of the two, and patient decisional conflict assessed at 2, 6, and 12 months post-intervention. Surrogate bereavement outcomes included anxiety, depression, and post-traumatic distress symptoms assessed at 2 weeks, and at 3 and 6 months after the patient's death.
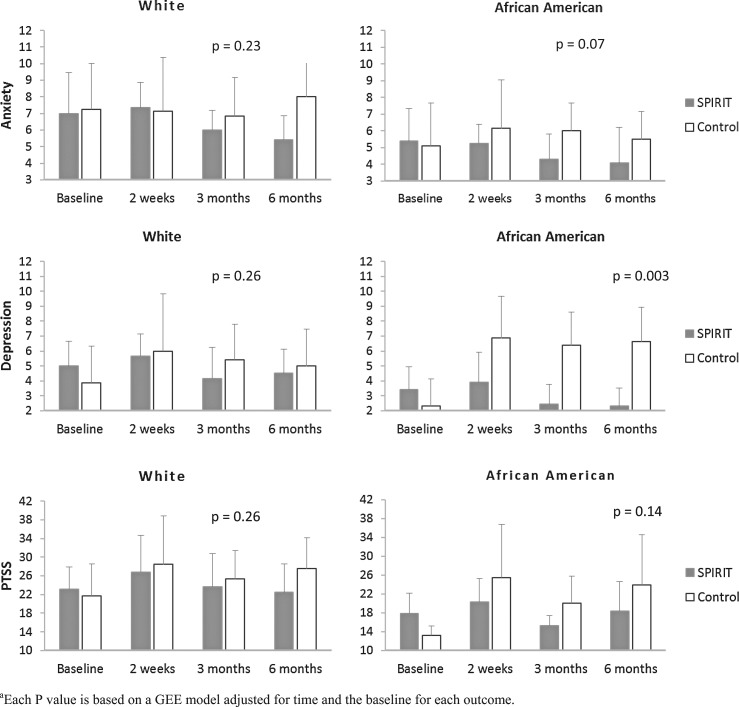
Results: SPIRIT was superior to usual care in improving dyad congruence (odds ration [OR] = 2.31, p = 0.018), surrogate decision-making confidence (β = 0.18, p = 0.021), and the composite (OR = 2.19, p = 0.028) 2 months post-intervention, but only for African Americans. SPIRIT reduced patient decisional conflict at 6 months for whites and at 12 months for African Americans. Finally, SPIRIT was superior to usual care in reducing surrogates' bereavement depressive symptoms for African Americans but not for whites (β = -3.49, p = 0.003).
Conclusion: SPIRIT was effective in improving preparation for end-of-life decision-making and post-bereavement outcomes in African Americans.
Figures
References
-
- U.S. Renal Data System. USRDS 2014 Annual Data Report: Epidemiology of Kidney Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2014
-
- Davison SN: Facilitating advance care planning for patients with end-stage renal disease: The patient perspectives. Clin J Am Soc Nephrol 2006;1:1023–1028 - PubMed
-
- Davison SN, Jhangri GS, Holley JL, Moss AH: Nephrologists' reported preparedness for end-of-life decision-making. Clin J Am Soc Nephrol 2006;1:1256–1262 - PubMed
-
- Renal Physicians Association: Shared Decision-making in the Appropriate Initiation of and Withdrawal from Dialysis: Clinical Practice Guideline, 2e. Renal Physicians Association, Rockville, MD, 2010
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
