

Highly sensitive troponin and coronary computed tomography angiography in the evaluation of suspected acute coronary syndrome in the emergency department
- PMID: 26843275
- PMCID: PMC6279199
- DOI: 10.1093/eurheartj/ehw005
Highly sensitive troponin and coronary computed tomography angiography in the evaluation of suspected acute coronary syndrome in the emergency department
Abstract
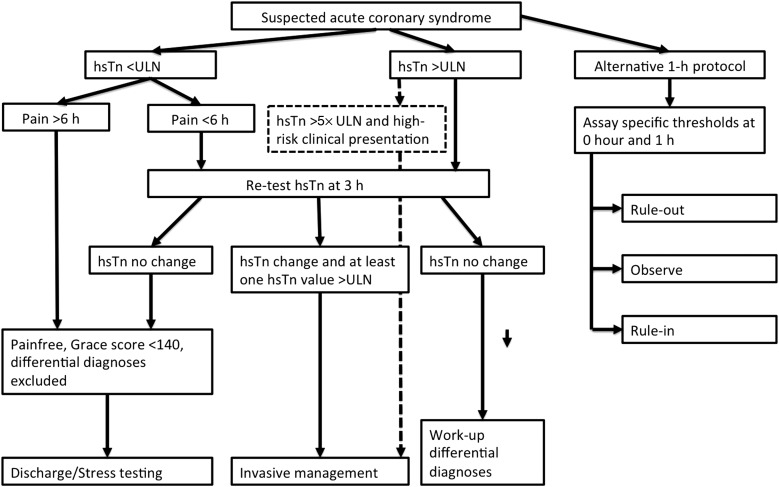
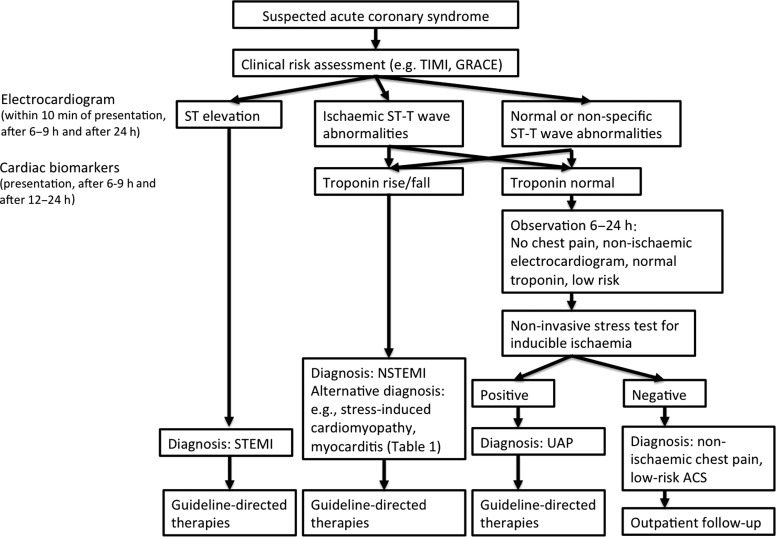
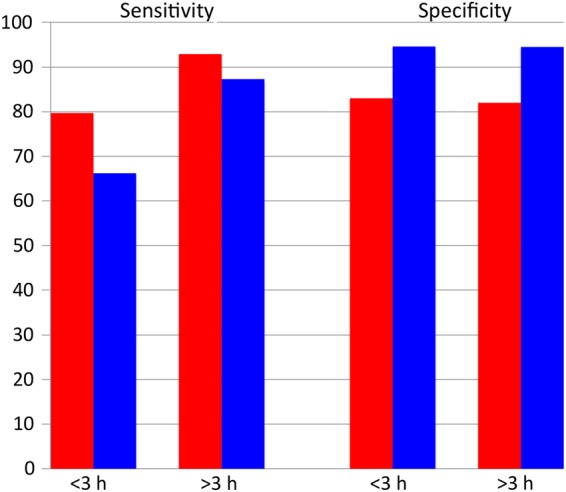
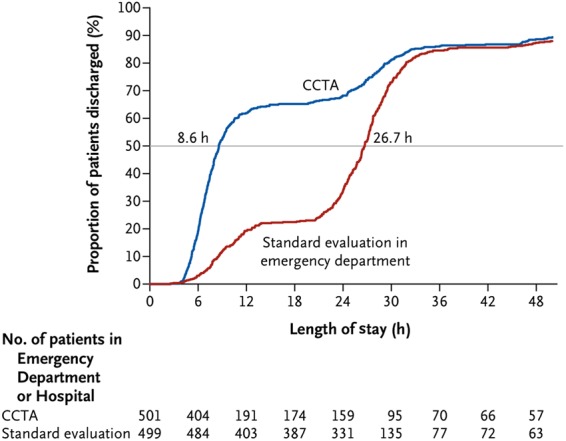
The evaluation of patients presenting to the emergency department with suspected acute coronary syndrome (ACS) remains a clinical challenge. The traditional assessment includes clinical risk assessment based on cardiovascular risk factors with serial electrocardiograms and cardiac troponin measurements, often followed by advanced cardiac testing as inpatient or outpatient (i.e. stress testing, imaging). Despite this costly and lengthy work-up, there is a non-negligible rate of missed ACS with an increased risk of death. There is a clinical need for diagnostic strategies that will lead to rapid and reliable triage of patients with suspected ACS. We provide an overview of the evidence for the role of highly sensitive troponin (hsTn) in the rapid and efficient evaluation of suspected ACS. Results of recent research studies have led to the introduction of hsTn with rapid rule-in and rule-out protocols into the guidelines. Highly sensitive troponin increases the sensitivity for the detection of myocardial infarction and decreases time to diagnosis; however, it may decrease the specificity, especially when used as a dichotomous variable, rather than continuous variable as recommended by guidelines; this may increase clinician uncertainty. We summarize the evidence for the use of coronary computed tomography angiography (CTA) as the rapid diagnostic tool in this population when used with conventional troponin assays. Coronary CTA significantly decreases time to diagnosis and discharge in patients with suspected ACS, while being safe. However, it may lead to increase in invasive procedures and includes radiation exposure. Finally, we outline the opportunities for the combined use of hsTn and coronary CTA that may result in increased efficiency, decreased need for imaging, lower cost, and decreased radiation dose.
Keywords: Acute chest pain; Acute coronary syndrome; Coronary computed tomography angiography; Highly sensitive troponin.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2016. For permissions please email: journals.permissions@oup.com.
Figures
Similar articles
-
hs-Troponin I Followed by CT Angiography Improves Acute Coronary Syndrome Risk Stratification Accuracy and Work-Up in Acute Chest Pain Patients: Results From ROMICAT II Trial.JACC Cardiovasc Imaging. 2015 Nov;8(11):1272-1281. doi: 10.1016/j.jcmg.2015.06.016. Epub 2015 Oct 14. JACC Cardiovasc Imaging. 2015. PMID: 26476506 Free PMC article. Clinical Trial.
-
Risk classification of highly sensitive troponin I predict presence of vulnerable plaque assessed by dual source coronary computed tomography angiography.Int J Cardiovasc Imaging. 2017 Nov;33(11):1831-1839. doi: 10.1007/s10554-017-1174-3. Epub 2017 May 20. Int J Cardiovasc Imaging. 2017. PMID: 28528430
-
Assessing sensitivity and specificity of the Manchester Triage System in the evaluation of acute coronary syndrome in adult patients in emergency care: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Nov;13(11):64-73. doi: 10.11124/jbisrir-2015-2213. JBI Database System Rev Implement Rep. 2015. PMID: 26657465
-
Is there still a role for cardiac CT in the emergency department in the era of highly-sensitive troponins?Minerva Cardioangiol. 2017 Jun;65(3):214-224. doi: 10.23736/S0026-4725.16.04291-2. Epub 2016 Nov 25. Minerva Cardioangiol. 2017. PMID: 27886161 Review.
-
[Cardiac troponins and beyond in acute coronary syndrome].Internist (Berl). 2019 Jun;60(6):555-563. doi: 10.1007/s00108-019-0611-x. Internist (Berl). 2019. PMID: 31076794 Review. German.
Cited by
-
The research progress and research trends in acute coronary syndrome nursing: A review of visual analysis based on the Web of Science database.Medicine (Baltimore). 2024 Feb 16;103(7):e35849. doi: 10.1097/MD.0000000000035849. Medicine (Baltimore). 2024. PMID: 38363951 Free PMC article. Review.
-
Coronary CT angiography for improved assessment of patients with acute chest pain and low-range positive high-sensitivity troponins: study protocol for a prospective, observational, multicentre study (COURSE trial).BMJ Open. 2021 Oct 18;11(10):e049349. doi: 10.1136/bmjopen-2021-049349. BMJ Open. 2021. PMID: 34663657 Free PMC article.
-
Development and validation of deep learning model for detection of obstructive coronary artery disease in patients with acute chest pain: a multi-center study.Radiol Med. 2025 Aug 14. doi: 10.1007/s11547-025-02064-1. Online ahead of print. Radiol Med. 2025. PMID: 40810889
-
Diagnosis of myocardial ischemia combining multiphase postmortem CT-angiography, histology, and postmortem biochemistry.Radiol Med. 2017 Feb;122(2):95-105. doi: 10.1007/s11547-016-0698-2. Epub 2016 Oct 20. Radiol Med. 2017. PMID: 27766573
References
-
- Niska R, Bhuiya F, Xu J. National Hospital Ambulatory Medical Care Survey: 2007 emergency department summary. Natl Health Stat Report 2010;1–31. Report No. 26. - PubMed
-
- McCaig LF, Burt CW. National Hospital Ambulatory Medical Care Survey: 2002 Emergency Department Summary. Advanced Data from Vital and Health Statistics. National Center for Health Statistics; 2004. pp. 1–36. Report No.: 340. - PubMed
-
- Pope JH, Aufderheide TP, Ruthazer R, Woolard RH, Feldman JA, Beshansky JR, Griffith JL, Selker HP. Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med 2000;342:1163–1170. - PubMed
-
- Swap CJ, Nagurney JT. Value and limitations of chest pain history in the evaluation of patients with suspected acute coronary syndromes. JAMA 2005;294:2623–2629. - PubMed
-
- Authors/Task Force Members Roffi M, Patrono C, Collet J-P, Mueller C, Valgimigli M, Andreotti F, Bax JJ, Borger MA, Brotons C, Chew DP, Gencer B, Hasenfuss G, Kjeldsen K, Lancellotti P, Landmesser U, Mehilli J, Mukherjee D, Storey RF, Windecker S. 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J 2015;1–59. [Epub ahead of print]. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
