

Coronary microcirculatory pathophysiology: can we afford it to remain a black box?
- PMID: 26843279
- PMCID: PMC5381591
- DOI: 10.1093/eurheartj/ehv760
Coronary microcirculatory pathophysiology: can we afford it to remain a black box?
Abstract
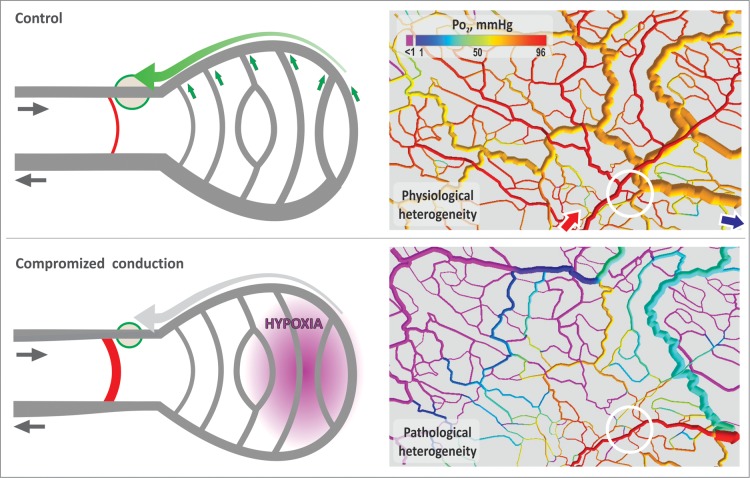
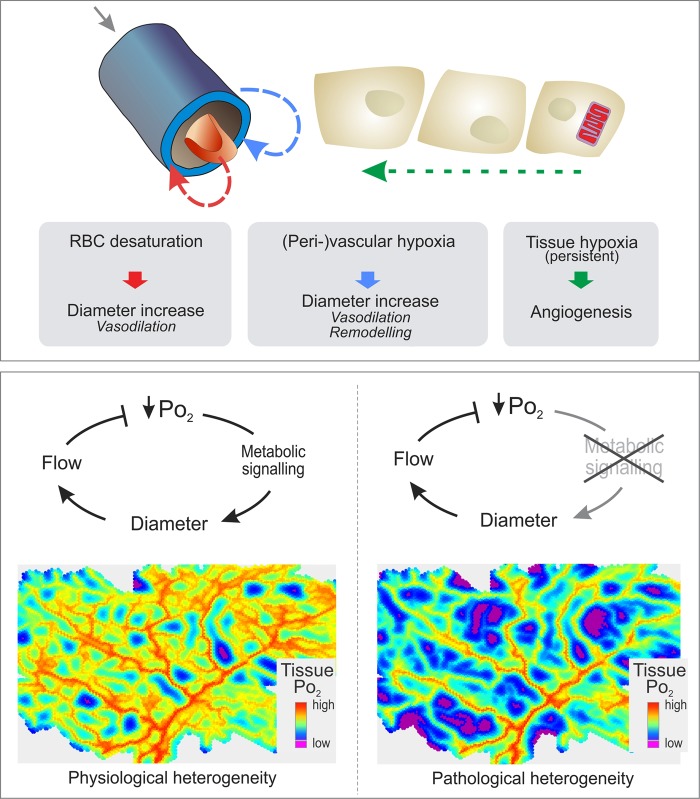
Coronary microvascular networks play the key role in determining blood flow distribution in the heart. Matching local blood supply to tissue metabolic demand entails continuous adaptation of coronary vessels via regulation of smooth muscle tone and structural dilated vessel diameter. The importance of coronary microcirculation for relevant pathological conditions including angina in patients with normal or near-normal coronary angiograms [microvascular angina (MVA)] and heart failure with preserved ejection fraction (HFpEF) is increasingly recognized. For MVA, clinical studies have shown a prevalence of up to 40% in patients with suspected coronary artery disease and a relevant impact on adverse cardiovascular events including cardiac death, stroke, and heart failure. Despite a continuously increasing number of corresponding clinical studies, the knowledge on pathophysiological cause-effect relations involving coronary microcirculation is, however, still very limited. A number of pathophysiological hypotheses for MVA and HFpEF have been suggested but are not established to a degree, which would allow definition of nosological entities, stratification of affected patients, or development of effective therapeutic strategies. This may be related to a steep decline in experimental (animal) pathophysiological studies in this area during the last 15 years. Since technology to experimentally investigate microvascular pathophysiology in the beating heart is increasingly, in principle, available, a concerted effort to build 'coronary microcirculatory observatories' to close this gap and to accelerate clinical progress in this area is suggested.
Keywords: CMVD; Conduction; Endothelial surface layer; Glycocalyx; HFpEF; MVA; Mathematical modelling; Metabolic regulation; Microvascular heterogeneity.
© The Author 2016. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures






References
-
- Likoff W, Segal BL, Kasparian H. Paradox of normal selective coronary arteriograms in patients considered to have unmistakable coronary heart disease. N Engl J Med 1967;276:1063–1066. - PubMed
-
- Cannon RO III, Epstein SE. “Microvascular angina” as a cause of chest pain with angiographically normal coronary arteries. Am J Cardiol 1988;61:1338–1343. - PubMed
-
- Lanza GA, Crea F. Primary coronary microvascular dysfunction: clinical presentation, pathophysiology, and management. Circulation 2010;121:2317–2325. - PubMed
-
- Johnston N, Schenck-Gustafsson K, Lagerqvist B. Are we using cardiovascular medications and coronary angiography appropriately in men and women with chest pain? Eur Heart J 2011;32:1331–1336. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
