

Phase II multicenter study of gene-mediated cytotoxic immunotherapy as adjuvant to surgical resection for newly diagnosed malignant glioma
- PMID: 26843484
- PMCID: PMC4933478
- DOI: 10.1093/neuonc/now002
Phase II multicenter study of gene-mediated cytotoxic immunotherapy as adjuvant to surgical resection for newly diagnosed malignant glioma
Abstract
Background: Despite aggressive standard of care (SOC) treatment, survival of malignant gliomas remains very poor. This Phase II, prospective, matched controlled, multicenter trial was conducted to assess the safety and efficacy of aglatimagene besadenovec (AdV-tk) plus valacyclovir (gene-mediated cytotoxic immunotherapy [GMCI]) in combination with SOC for newly diagnosed malignant glioma patients.
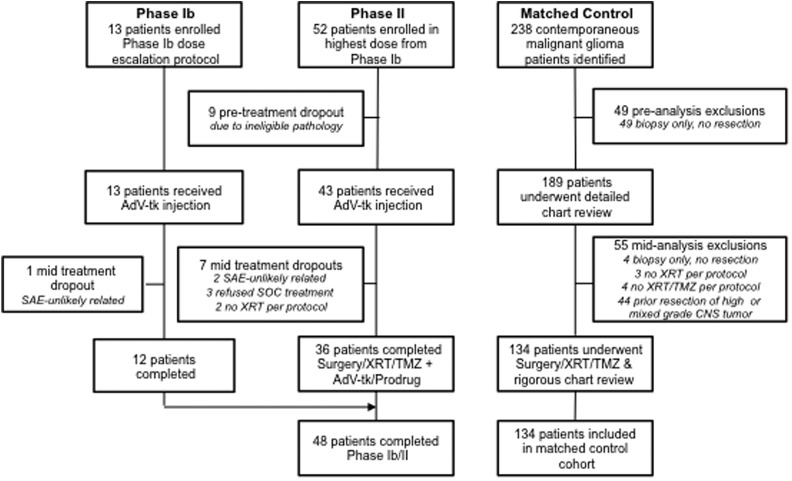
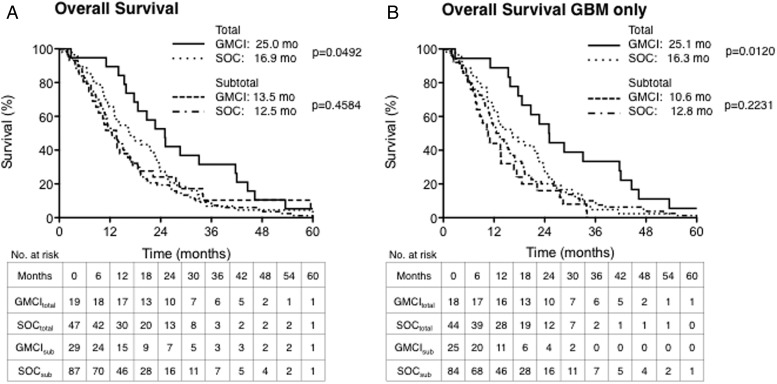
Methods: Treatment cohort patients received SOC + GMCI and were enrolled at 4 institutions from 2006 to 2010. The preplanned, matched-control cohort included all concurrent patients meeting protocol criteria and SOC at a fifth institution. AdV-tk was administered at surgery followed by SOC radiation and temozolomide. Subset analyses were preplanned, based on prognostic factors: pathological diagnosis (glioblastoma vs others) and extent of resection.
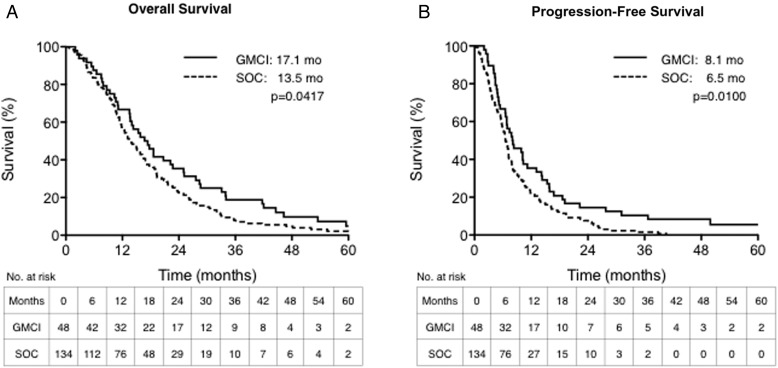
Results: Forty-eight patients completed SOC + GMCI, and 134 met control cohort criteria. Median overall survival (OS) was 17.1 months for GMCI + SOC versus 13.5 months for SOC alone (P = .0417). Survival at 1, 2, and 3 years was 67%, 35%, and 19% versus 57%, 22%, and 8%, respectively. The greatest benefit was observed in gross total resection patients: median OS of 25 versus 16.9 months (P = .0492); 1, 2, and 3-year survival of 90%, 53%, and 32% versus 64%, 28% and 6%, respectively. There were no dose-limiting toxicities; fever, fatigue, and headache were the most common GMCI-related symptoms.
Conclusions: GMCI can be safely combined with SOC in newly diagnosed malignant gliomas. Survival outcomes were most notably improved in patients with minimal residual disease after gross total resection. These data should help guide future immunotherapy studies and strongly support further evaluation of GMCI for malignant gliomas.
Clinical trial registry: ClinicalTrials.gov NCT00589875.
Keywords: gene therapy; glioblastoma; immuno-oncology; immunotherapy; malignant glioma.
© The Author(s) 2016. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Wen PY, Kesari S. Malignant gliomas in adults. N Engl J Med. 2008;359(17):492–507. - PubMed
-
- Stupp R, Hegi ME, Mason WP et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10(5):459–466. - PubMed
-
- Kreth F-W, Thon N, Simon M et al. Gross total but not incomplete resection of glioblastoma prolongs survival in the era of radiochemotherapy. Ann Oncol. 2013;24(12):3117–3123. - PubMed
-
- Grabowski MM, Recinos PF, Nowacki AS et al. Residual tumor volume versus extent of resection: predictors of survival after surgery for glioblastoma. J Neurosurg. 2014;121(5):1115–1123. - PubMed
-
- Aguilar LK, Guzik BW, Aguilar-Cordova E. Cytotoxic immunotherapy strategies for cancer: mechanisms and clinical development. J Cell Biochem. 2011;112(8):1969–1977. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
