

Gallstone ileus, clinical presentation, diagnostic and treatment approach
- PMID: 26843914
- PMCID: PMC4724589
- DOI: 10.4240/wjgs.v8.i1.65
Gallstone ileus, clinical presentation, diagnostic and treatment approach
Abstract
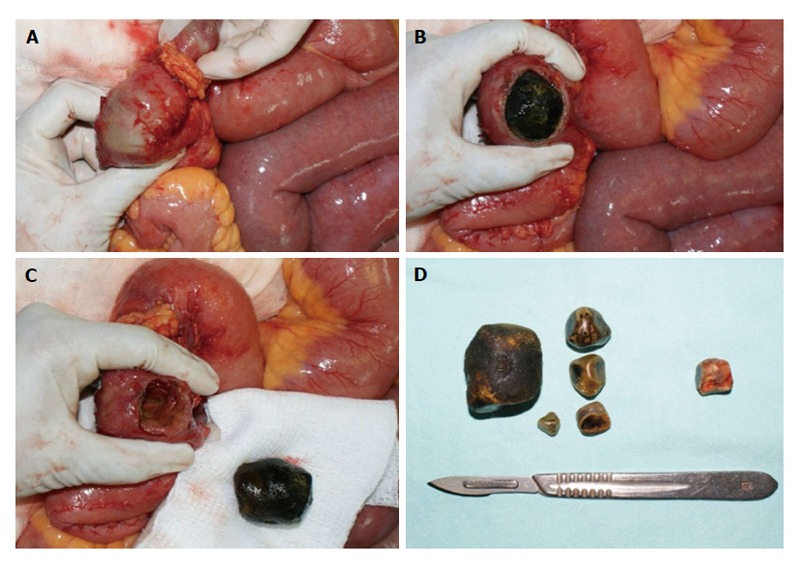
Gallstone ileus is a mechanical intestinal obstruction due to gallstone impaction within the gastrointestinal tract. Less than 1% of cases of intestinal obstruction are derived from this etiology. The symptoms and signs of gallstone ileus are mostly nonspecific. This entity has been observed with a higher frequency among the elderly, the majority of which have concomitant medical illness. Cardiovascular, pulmonary, and metabolic diseases should be considered as they may affect the prognosis. Surgical relief of gastrointestinal obstruction remains the mainstay of operative treatment. The current surgical procedures are: (1) simple enterolithotomy; (2) enterolithotomy, cholecystectomy and fistula closure (one-stage procedure); and (3) enterolithotomy with cholecystectomy performed later (two-stage procedure). Bowel resection is necessary in certain cases after enterolithotomy is performed. Large prospective laparoscopic and endoscopic trials are expected.
Keywords: Bouveret’s syndrome; Endoscopic treatment; Gallstone ileus; Intestinal obstruction; Laparoscopic surgery.
Figures

References
-
- Abou-Saif A, Al-Kawas FH. Complications of gallstone disease: Mirizzi syndrome, cholecystocholedochal fistula, and gallstone ileus. Am J Gastroenterol. 2002;97:249–254. - PubMed
-
- Courvoisier LG. Casuistisch-statistische Beitrage zur Pathologic und Chirurgie der gallenwege. XII Leipzig, FCW Vogel: 1890.
-
- Bouveret L. Stenose du pylore adherent a la vesicule calculeuse. Rev Med (Paris) 1896;16:1–16.
-
- Kurtz RJ, Heimann TM, Beck AR, Kurtz AB. Patterns of treatment of gallstone ileus over a 45-year period. Am J Gastroenterol. 1985;80:95–98. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
