

Economics and Outcome After Hematopoietic Stem Cell Transplantation: A Retrospective Cohort Study
- PMID: 26844291
- PMCID: PMC4703735
- DOI: 10.1016/j.ebiom.2015.11.021
Economics and Outcome After Hematopoietic Stem Cell Transplantation: A Retrospective Cohort Study
Abstract
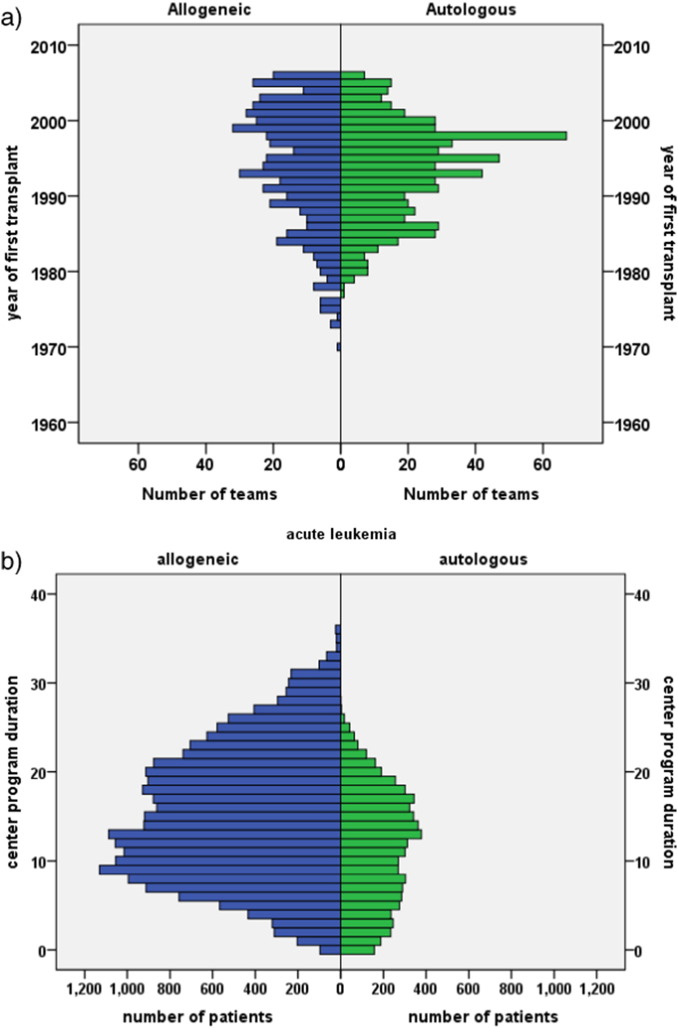
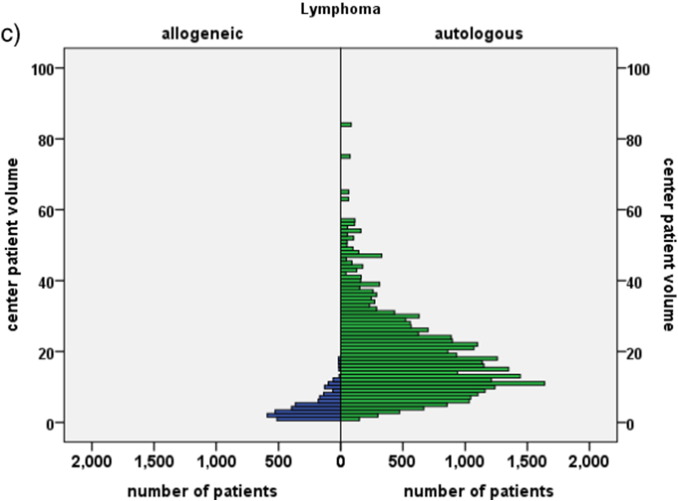
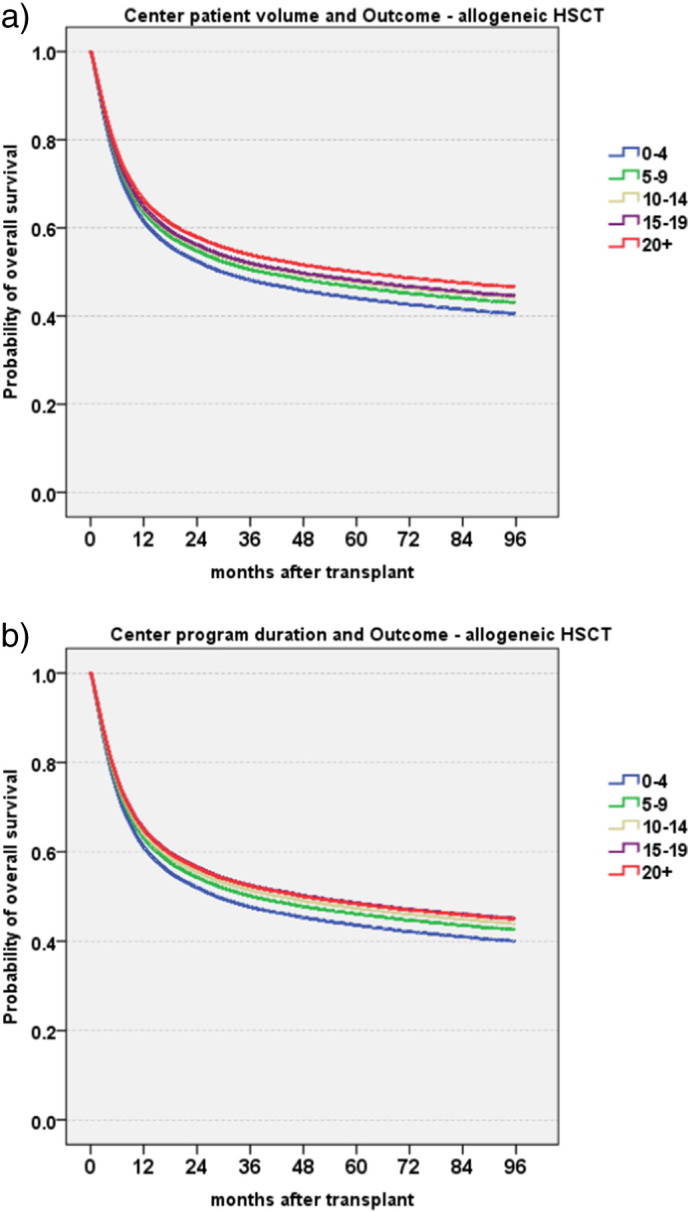
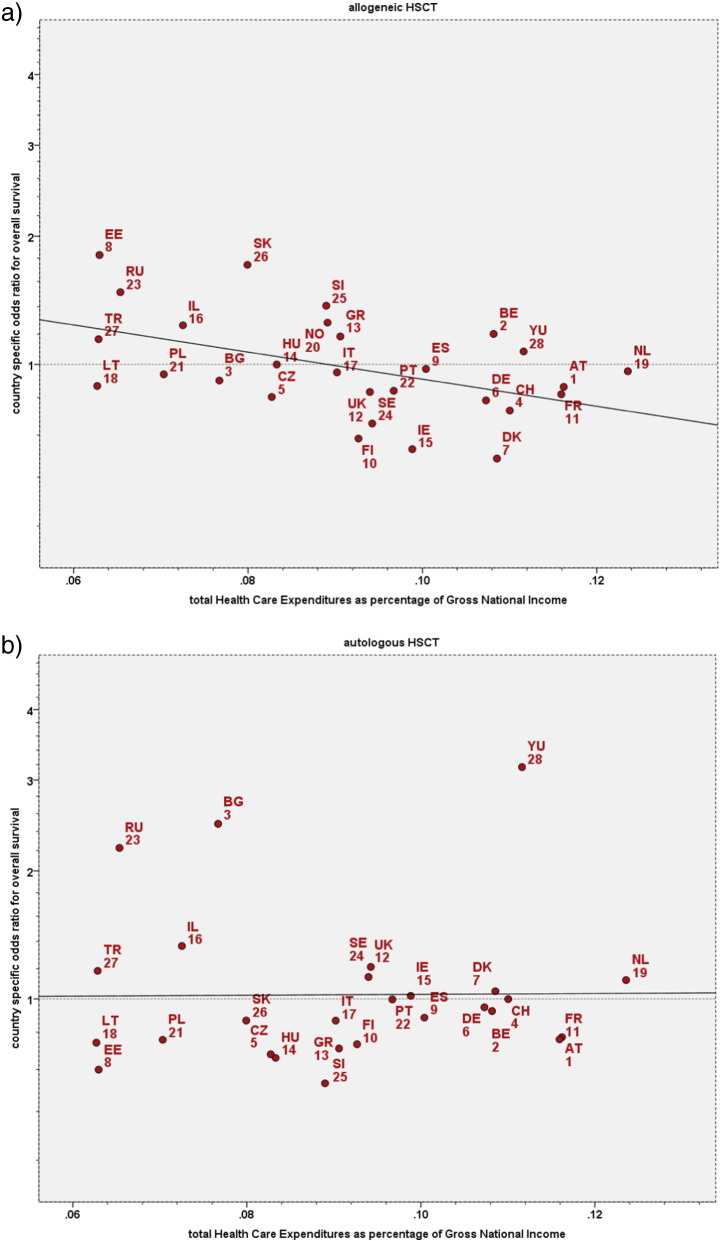
Hematopoietic stem cell transplantation (HSCT) is a lifesaving expensive medical procedure. Hence, more transplants are performed in more affluent countries. The impact of economic factors on patient outcome is less defined. We analyzed retrospectively a defined cohort of 102,549 patients treated with an allogeneic (N = 37,542; 37%) or autologous (N = 65,007; 63%) HSCT. They were transplanted by one of 404 HSCT centers in 25 European countries between 1999 and 2006. We searched for associations between center-specific microeconomic or country-specific macroeconomic factors and outcome. Center patient-volume and center program-duration were significantly and systematically associated with improved survival after allogeneic HSCT (HR 0·87; 0·84-0·91 per 10 patients; p < 0·0001; HR 0·90;0·85-0·90 per 10 years; p < 0·001) and autologous HSCT (HR 0·91;0·87-0·96 per 10 patients; p < 0·001; HR 0·93;0·87-0·99 per 10 years; p = 0·02). The product of Health Care Expenditures by Gross National Income/capita was significantly associated in multivariate analysis with all endpoints (R(2) = 18%; for relapse free survival) after allogeneic HSCT. Data indicate that country- and center-specific economic factors are associated with distinct, significant, systematic, and clinically relevant effects on survival after HSCT. They impact on center expertise in long-term disease and complication management. It is likely that these findings apply to other forms of complex treatments.
Keywords: Center effect; GNI/cap; HCE/cap; HDI; Hematopoietic stem cell transplantation; Macroeconomics; Microeconomics; Outcome; Patient volume; Program duration; Risk assessment; Survival.
Figures
Comment in
-
Beyond Biology: Impact of Center- and Country-specific Economic Factors on Outcomes After Hematopoietic Cell Transplantation.EBioMedicine. 2015 Dec 12;2(12):1869-70. doi: 10.1016/j.ebiom.2015.12.005. eCollection 2015 Dec. EBioMedicine. 2015. PMID: 26844265 Free PMC article. No abstract available.
References
-
- Waitzkin H. Report of the WHO Commission on Macroeconomics and Health: a summary and critique. Lancet. 2003;361:523–526. - PubMed
-
- Gratwohl A., Pasquini M.C., Aljurf M. For the Worldwide Network of Blood and Marrow Transplantation WBMT. One million haemopoietic stem-cell transplants: a retrospective observational study. Lancet Haematol. 2015;2:e91–100. - PubMed
-
- Copelan E.A. Hematopoietic stem-cell transplantation. N. Engl. J. Med. 2006;354:1813–1826. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
