

Differential Effects of Bariatric Surgery Versus Exercise on Excessive Visceral Fat Deposits
- PMID: 26844473
- PMCID: PMC4748890
- DOI: 10.1097/MD.0000000000002616
Differential Effects of Bariatric Surgery Versus Exercise on Excessive Visceral Fat Deposits
Abstract
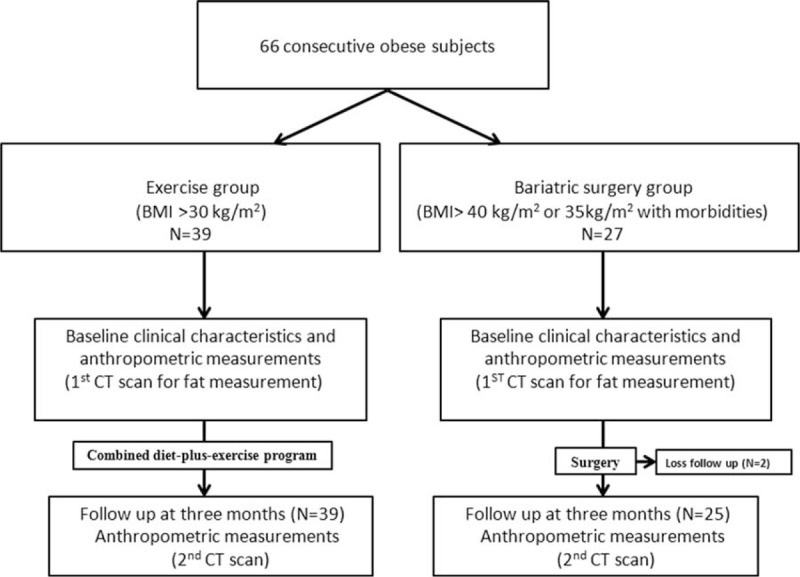
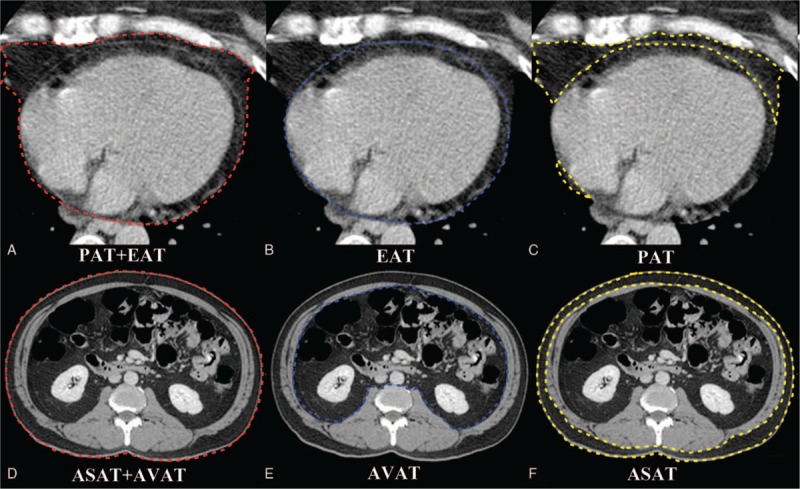
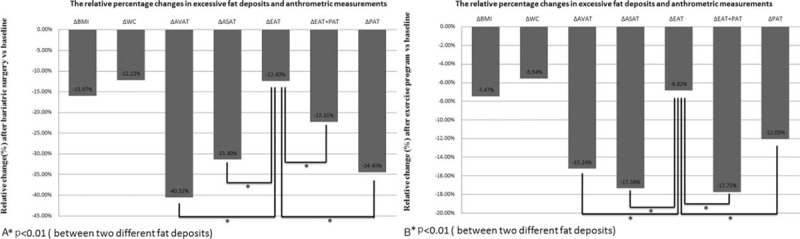
The aim of the present study was to compare differential impacts of bariatric surgery and exercise-induced weight loss on excessive abdominal and cardiac fat deposition.Excessive fat accumulation around the heart may play an important role in the pathogenesis of cardiovascular disease. Recent evidences have suggested that bariatric surgery results in relatively less decrease in epicardial fat compared with abdominal visceral fat and paracardial fat.Sixty-four consecutive overweight or obese subjects were enrolled in the study. Clinical characteristics and metabolic profiles were recorded. The volumes of abdominal visceral adipose tissue (AVAT), abdominal subcutaneous adipose tissue (ASAT), epicardial (EAT), and paracardial adipose tissue (PAT) were measured by computed tomography in the bariatric surgery group (N = 25) and the exercise group (N = 39) at baseline and 3 months after intervention. Subjects in both the surgery and exercise groups showed significant reduction in body mass index (15.97%, 7.47%), AVAT (40.52%, 15.24%), ASAT (31.40, 17.34%), PAT (34.40%, 12.05%), and PAT + EAT (22.31%, 17.72%) (all P < 0.001) after intervention compared with baseline. In both the groups, the decrease in EAT was small compared with the other compartments (P < 0.01 in both groups). Compared with the exercise group, the surgery group had greater loss in abdominal and cardiac visceral adipose tissue (AVAT, ASAT, PAT, EAT+PAT) (P < 0.001), but lesser loss in EAT (P = 0.037).Compared with the exercise group, bariatric surgery results in significantly greater percentage loss of excessive fat deposits except for EAT. EAT, but not PAT, was relatively preserved despite weight reduction in both the groups. The physiological impact of persistent EAT deserves further investigation.
Conflict of interest statement
The authors have no conflicts of interest to disclose. The authors report no potential conflicts of interest with any companies or organizations whose products or services are mentioned in this article.
Figures
References
-
- Picot J, Jones J, Colquitt JL, et al. The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: a systematic review and economic evaluation. Health Technol Assess 2009; 13:214. - PubMed
-
- Despres J-P, Lemieux I. Abdominal obesity and metabolic syndrome. Nature 2006; 444:881–887. - PubMed
-
- Després J-P, Lemieux I, Bergeron J, et al. Abdominal obesity and the metabolic syndrome: contribution to global cardiometabolic risk. Arterioscler Thromb Vasc Biol 2008; 28:1039–1049. - PubMed
-
- Chaston TB, Dixon JB. Factors associated with percent change in visceral versus subcutaneous abdominal fat during weight loss: findings from a systematic review. Int J Obes 2008; 32:619–628. - PubMed
-
- Sacks HS, Fain JN. Human epicardial adipose tissue: a review. Am Heart J 2007; 153:907–917. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
