

Recent Trends in Hospitalization for Acute Myocardial Infarction in Beijing: Increasing Overall Burden and a Transition From ST-Segment Elevation to Non-ST-Segment Elevation Myocardial Infarction in a Population-Based Study
- PMID: 26844503
- PMCID: PMC4748920
- DOI: 10.1097/MD.0000000000002677
Recent Trends in Hospitalization for Acute Myocardial Infarction in Beijing: Increasing Overall Burden and a Transition From ST-Segment Elevation to Non-ST-Segment Elevation Myocardial Infarction in a Population-Based Study
Abstract
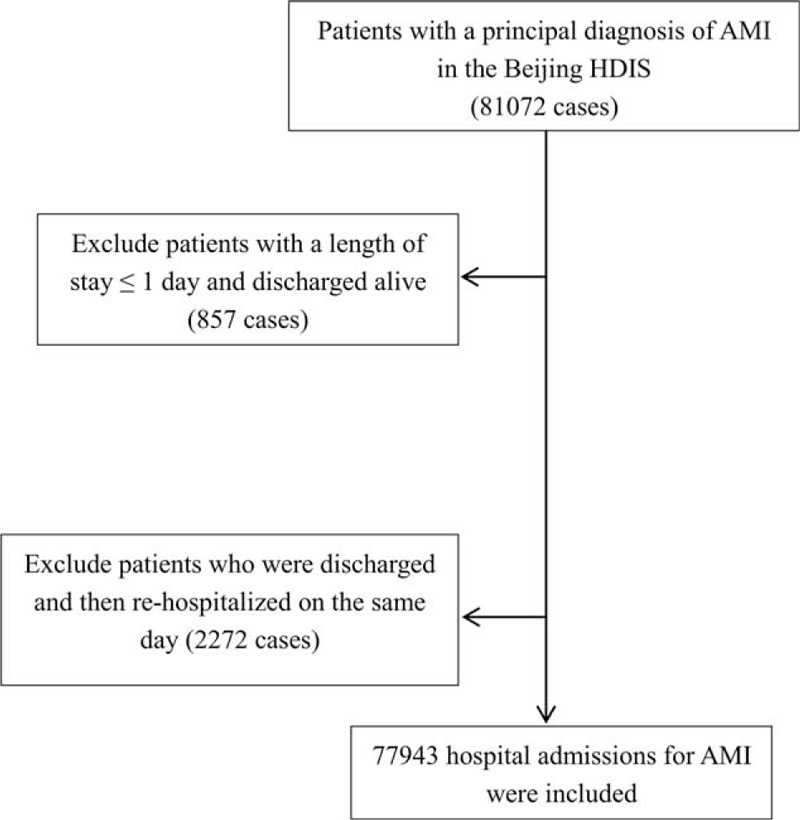
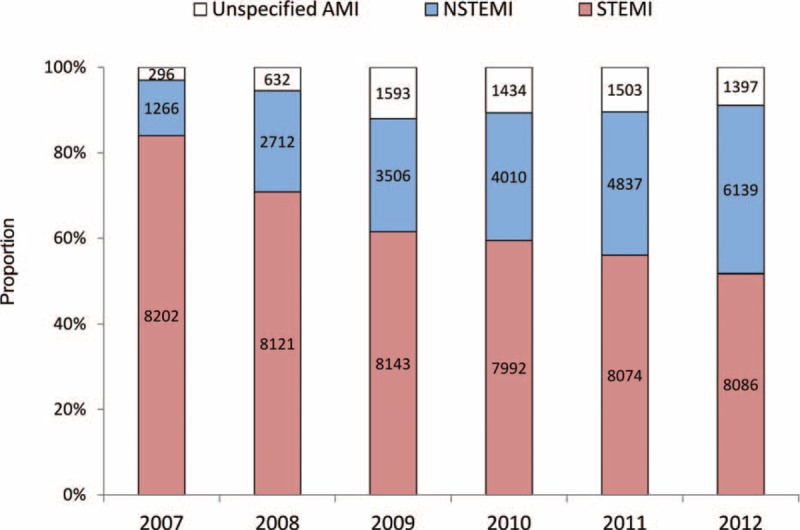
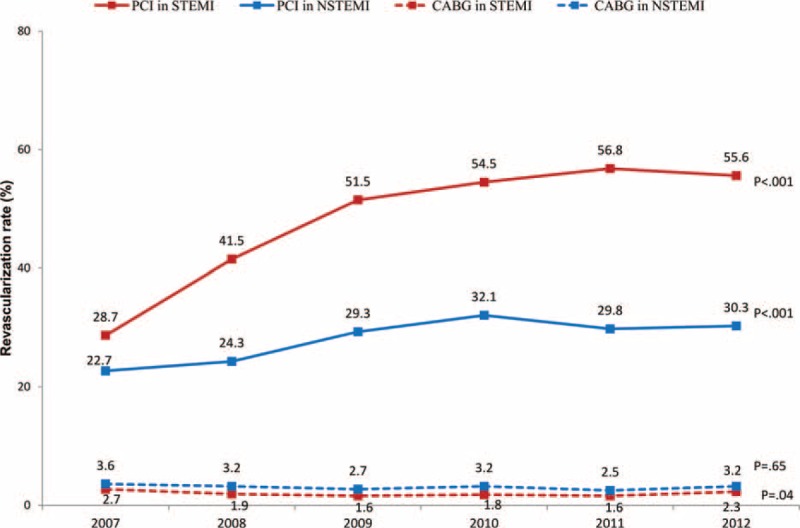
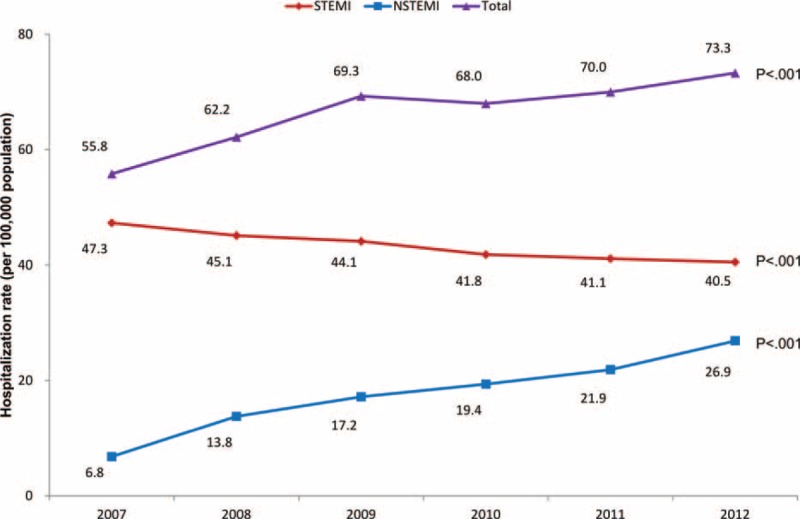
Comparable data on trends of hospitalization rates for ST-segment elevation myocardial infarction (STEMI) and non-STEMI (NSTEMI) remain unavailable in representative Asian populations.To examine the temporal trends of hospitalization for acute myocardial infarction (AMI) and its subtypes in Beijing.Patients hospitalized for AMI in Beijing from January 1, 2007 to December 31, 2012 were identified from the validated Hospital Discharge Information System. Trends in hospitalization rates, in-hospital mortality, length of stay (LOS), and hospitalization costs were analyzed by regression models for total AMI and for STEMI and NSTEMI separately. In total, 77,943 patients were admitted for AMI in Beijing during the 6 years, among whom 67.5% were males and 62.4% had STEMI. During the period, the rate of AMI hospitalization per 100,000 population increased by 31.2% (from 55.8 to 73.3 per 100,000 population) after age standardization, with a slight decrease in STEMI but a 3-fold increase in NSTEMI. The ratio of STEMI to NSTEMI decreased dramatically from 6.5:1.0 to 1.3:1.0. The age-standardized in-hospital mortality decreased from 11.2% to 8.6%, with a significant decreasing trend evident for STEMI in males and females (P < 0.001) and for NSTEMI in males (P = 0.02). The rate of percutaneous coronary intervention increased from 28.7% to 55.6% among STEMI patients. The total cost for AMI hospitalization increased by 56.8% after adjusting for inflation, although the LOS decreased by 1 day.The hospitalization burden for AMI has been increasing in Beijing with a transition from STEMI to NSTEMI. Diverse temporal trends in AMI subtypes from the unselected "real-world" data in Beijing may help to guide the management of AMI in China and other developing countries.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
[Trends in 30-day case fatality rate in patients hospitalized due to acute myocardial infarction in Beijing, 2007-2012].Zhonghua Liu Xing Bing Xue Za Zhi. 2018 Mar 10;39(3):363-367. doi: 10.3760/cma.j.issn.0254-6450.2018.03.022. Zhonghua Liu Xing Bing Xue Za Zhi. 2018. PMID: 29609255 Chinese.
-
[Trends of in-hospital mortality and constituent ratio of patients with acute myocardial infarction].Zhonghua Xin Xue Guan Bing Za Zhi. 2019 Mar 24;47(3):209-214. doi: 10.3760/cma.j.issn.0253-3758.2019.03.006. Zhonghua Xin Xue Guan Bing Za Zhi. 2019. PMID: 30897880 Chinese.
-
Trends in hospitalisation for acute myocardial infarction in Ireland, 1997-2008.Heart. 2012 Sep;98(17):1285-9. doi: 10.1136/heartjnl-2012-301822. Epub 2012 Jul 16. Heart. 2012. PMID: 22802000
-
Influence of daily temperature on the occurrence of ST-elevation myocardial infarction.J Cardiol. 2023 Jun;81(6):544-552. doi: 10.1016/j.jjcc.2022.12.005. Epub 2022 Dec 21. J Cardiol. 2023. PMID: 36565995 Review.
-
Italian contributions to the history of acute myocardial infarction treatment.Minerva Cardiol Angiol. 2024 Feb;72(1):32-40. doi: 10.23736/S2724-5683.23.06335-4. Epub 2023 Jun 13. Minerva Cardiol Angiol. 2024. PMID: 37310157 Review.
Cited by
-
Prognostic Value of Metabolic Syndrome in Patients With Non-ST Elevated Myocardial Infarction Undergoing Percutaneous Coronary Intervention.Front Cardiovasc Med. 2022 Jun 23;9:912999. doi: 10.3389/fcvm.2022.912999. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35811732 Free PMC article.
-
Impact of Sex- and Gender-Related Factors on Length of Stay Following Non-ST-Segment-Elevation Myocardial Infarction: A Multicountry Analysis.J Am Heart Assoc. 2023 Aug;12(15):e028553. doi: 10.1161/JAHA.122.028553. Epub 2023 Jul 25. J Am Heart Assoc. 2023. PMID: 37489737 Free PMC article.
-
Epidemiology and current management of cardiovascular disease in China.J Geriatr Cardiol. 2024 Apr 28;21(4):387-406. doi: 10.26599/1671-5411.2024.04.001. J Geriatr Cardiol. 2024. PMID: 38800543 Free PMC article.
-
Patients with ST-segment elevation of myocardial infarction miss out on early reperfusion: when to undergo delayed revascularization.J Geriatr Cardiol. 2017 Aug;14(8):524-531. doi: 10.11909/j.issn.1671-5411.2017.08.006. J Geriatr Cardiol. 2017. PMID: 29089969 Free PMC article.
-
Geographic Variation in Mortality of Acute Myocardial Infarction and Association With Health Care Accessibility in Beijing, 2007 to 2018.J Am Heart Assoc. 2023 Jun 20;12(12):e029769. doi: 10.1161/JAHA.123.029769. Epub 2023 Jun 10. J Am Heart Assoc. 2023. PMID: 37301748 Free PMC article.
References
-
- Freisinger E, Fuerstenberg T, Malyar NM, et al. German nationwide data on current trends and management of acute myocardial infarction: discrepancies between trials and real-life. Eur Heart J 2014; 35:979–988. - PubMed
-
- Jennings SM, Bennett K, Lonergan M, et al. Trends in hospitalisation for acute myocardial infarction in Ireland, 1997–2008. Heart 2012; 98:1285–1289. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
