

Managing Epilepsy in Women
- PMID: 26844738
- PMCID: PMC8734579
- DOI: 10.1212/CON.0000000000000270
Managing Epilepsy in Women
Abstract
Purpose of review: Caring for a woman with epilepsy requires familiarity with the implications of antiepileptic drugs (AEDs) for pregnancy and contraception as well as an understanding of the effects of female hormones on epilepsy.
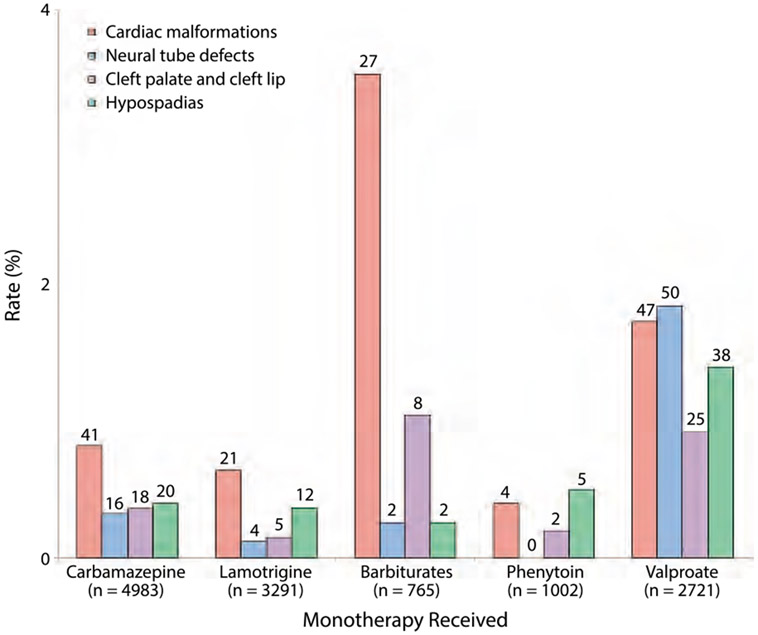
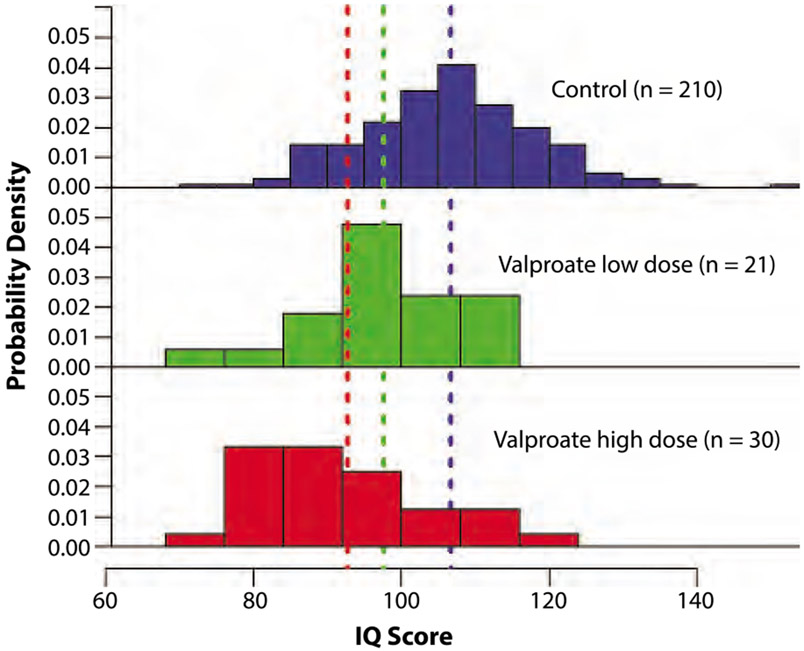
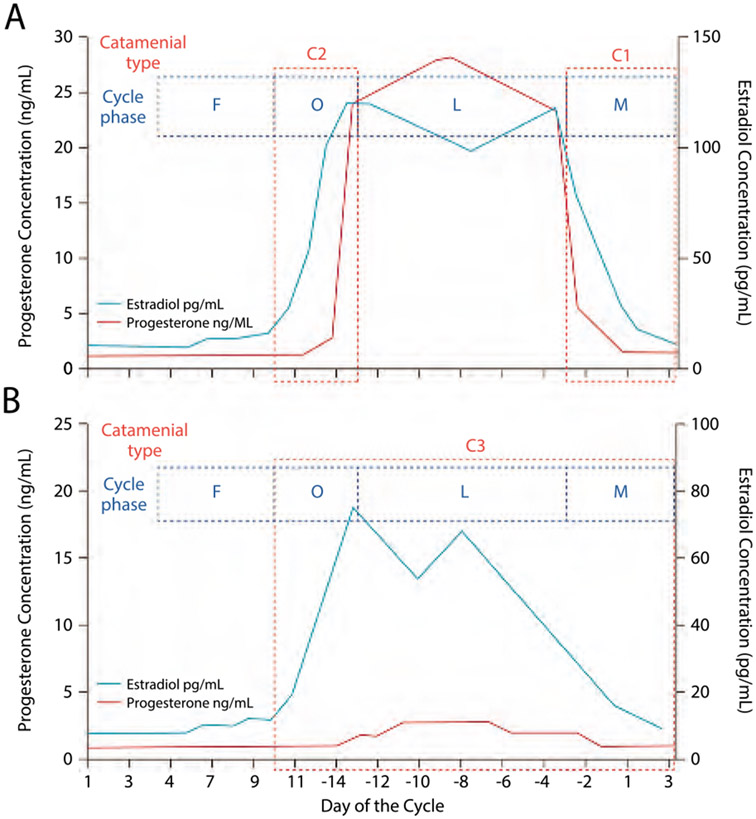
Recent findings: AED pregnancy registries and prospective studies of cognitive development continue to confirm that valproate poses a significantly increased risk of structural and cognitive teratogenesis. In contrast, data thus far suggest that lamotrigine and levetiracetam are associated with a relatively low risk for both anatomic and developmental adverse effects, although further studies are needed for these and other AEDs. The intrauterine device is a good contraceptive option for many women with epilepsy as it is highly effective and not subject to the drug-drug interactions seen between hormonal contraception and many AEDs. Hormonal-sensitive seizures are common among women with epilepsy; however, highly effective treatments for refractory catamenial seizures are limited.
Summary: Women with epilepsy should be counseled early and regularly about reproductive health as it relates to epilepsy. AED selection for women of childbearing age should take future pregnancies and contraceptive needs into consideration.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical