

Digital interventions to promote self-management in adults with hypertension systematic review and meta-analysis
- PMID: 26845284
- PMCID: PMC4947544
- DOI: 10.1097/HJH.0000000000000859
Digital interventions to promote self-management in adults with hypertension systematic review and meta-analysis
Abstract
Objective: To synthesize the evidence for using interactive digital interventions (IDIs) to support patient self-management of hypertension, and to determine their impact on control and reduction of blood pressure.
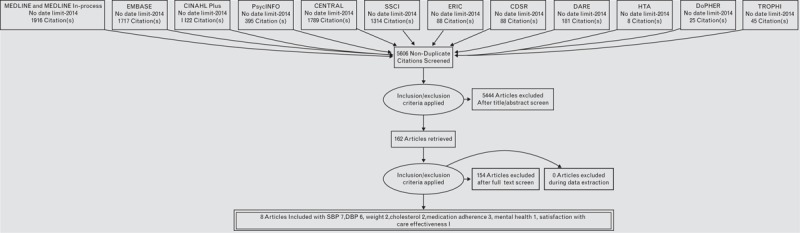
Method: Systematic review with meta-analysis was undertaken with a search performed in MEDLINE, EMBASE, CINAHL, PsycINFO, ERIC, Cochrane Library, DoPHER, TROPHI, Social Science Citation Index and Science Citation Index. The population was adults (>18 years) with hypertension, intervention was an IDI and the comparator was usual care. Primary outcomes were change in SBP and DBP. Only randomized controlled trials and studies published in journals and in English were eligible. Eligible IDIs included interventions accessed through a computer, smartphone or other hand-held device.
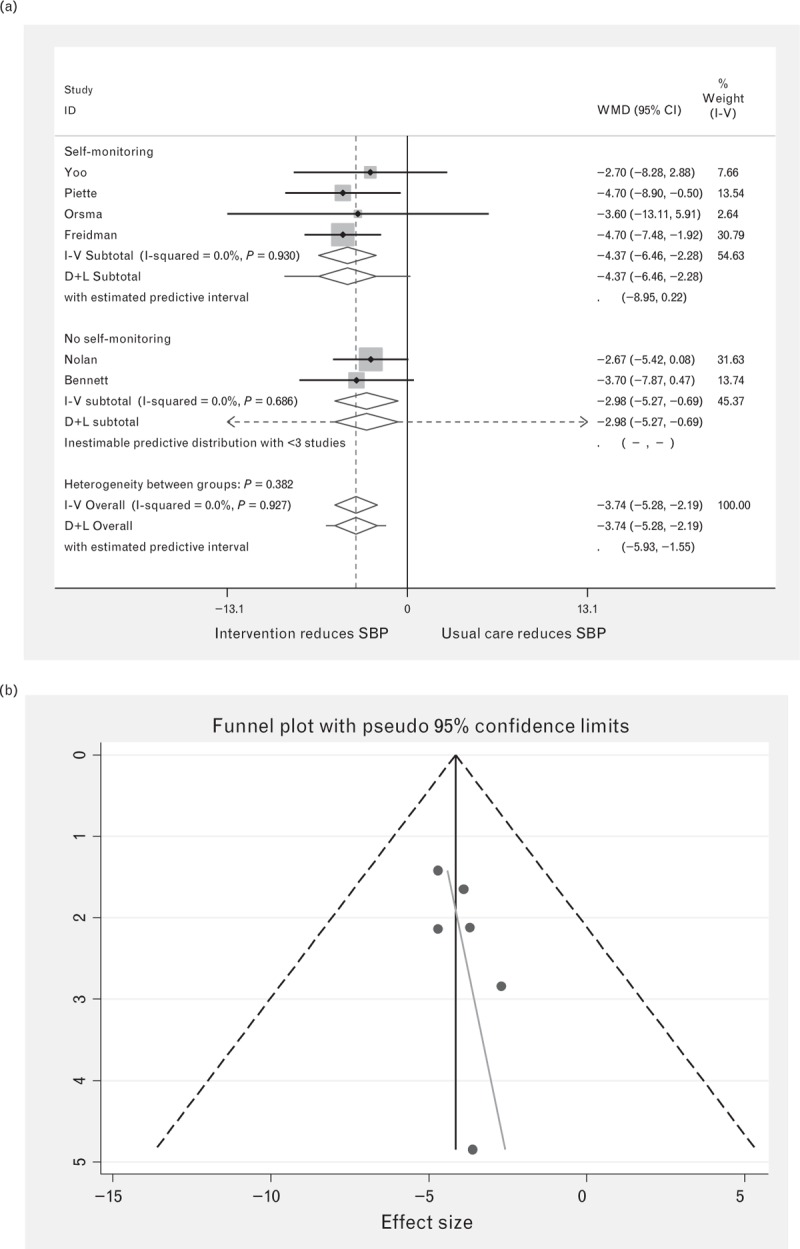
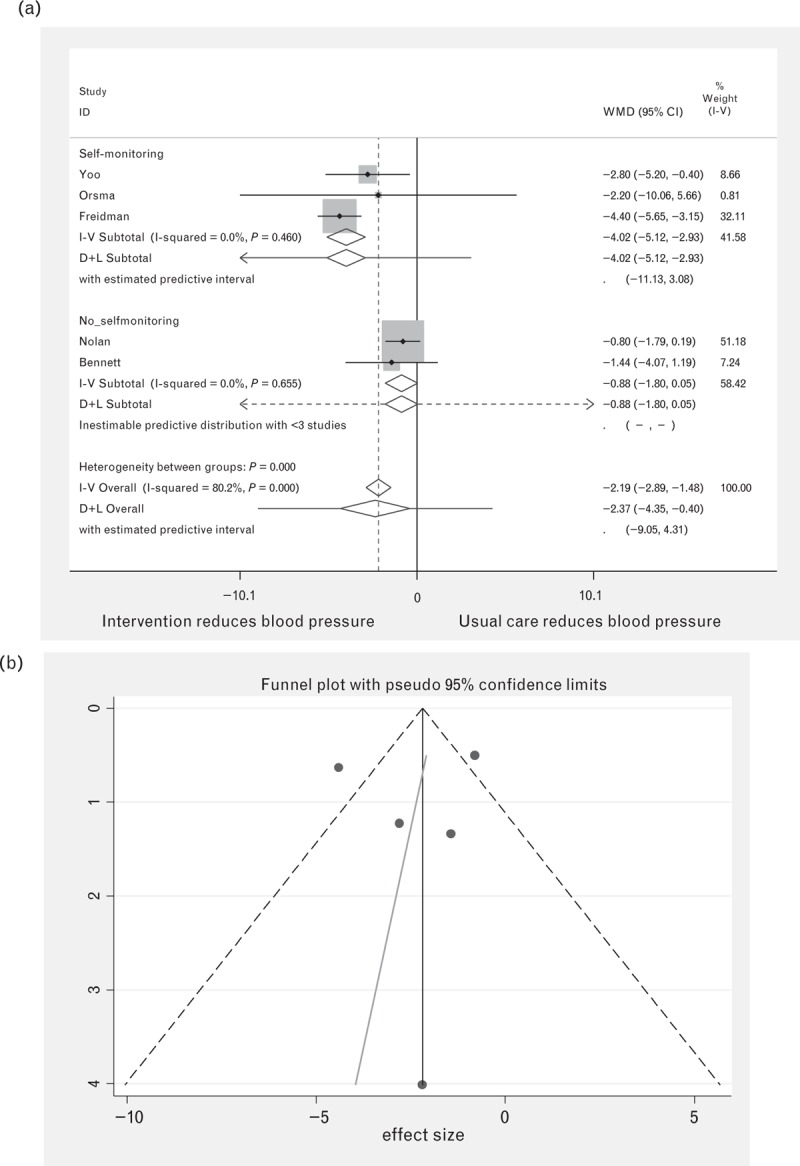
Results: Four out of seven studies showed a significantly greater reduction for intervention compared to usual care for SBP, with no difference found for three. Overall, IDIs significantly reduced SBP, with the weighted mean difference being -3.74 mmHg [95% confidence interval (CI) -2.19 to -2.58] with no heterogeneity observed (I-squared = 0.0%, P = 0.990). For DBP, four out of six studies indicated a greater reduction for intervention compared to controls, with no difference found for two. For DBP, a significant reduction of -2.37 mmHg (95% CI -0.40 to -4.35) was found, but considerable heterogeneity was noted (I-squared = 80.1%, P = <0.001).
Conclusion: IDIs lower both SBP and DBP compared to usual care. Results suggest these findings can be applied to a wide range of healthcare systems and populations. However, sustainability and long-term clinical effectiveness of these interventions remain uncertain.
Figures
References
-
- Wang H, Dwyer-Lindgren L, Lofgren KT, Rajaratnam JK, Marcus JR, Levin-Rector A, et al. Age-specific and sex-specific mortality in 187 countries, 1970–2010: a systematic analysis for the Global Burden of Disease Study. Lancet 2012; 380:2071–2094. - PubMed
-
- Stamler J, Stamler R, Neaton JD. Blood pressure, systolic and diastolic, and cardiovascular risks: US population data. Arch Intern Med 1993; 153:598–615. - PubMed
-
- Collins R, Peto R, MacMahon S, Hebert P, Fiebach NH, Eberlein KA, et al. Blood pressure, stroke, and coronary heart disease. Part 2. Short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet 1990; 335:827–838. - PubMed
-
- Chow CK, Teo KK, Rangarajan S, Islam S, Gupta R, Avezum A, Bahonar A. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA 2013; 310:959–968. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
