

Reducing antibiotic prescriptions for respiratory tract infections in family practice: results of a cluster randomized controlled trial evaluating a multifaceted peer-group-based intervention
- PMID: 26845640
- PMCID: PMC4741286
- DOI: 10.1038/npjpcrm.2015.83
Reducing antibiotic prescriptions for respiratory tract infections in family practice: results of a cluster randomized controlled trial evaluating a multifaceted peer-group-based intervention
Abstract
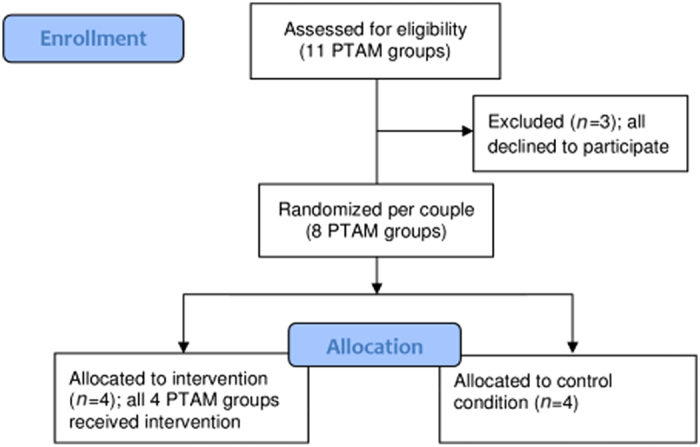
Irrational antibiotic use for respiratory tract infections (RTI) is a major driver of bacterial resistance. The aim of this study was to evaluate the effect of a multifaceted peer-group based intervention aiming to reduce RTI-related antibiotic prescriptions in family practice. This was a cluster randomized controlled trial with pre- and follow-up measurement. The intervention was implemented through PharmacoTherapy Audit Meetings (PTAM) in which family physicians (FPs) and pharmacists collaborate. Four PTAM groups received the intervention consisting of: (1) FP communication skills training, including communication about delayed prescribing; (2) implementation of antibiotic prescribing agreements in FPs' Electronic Prescribing Systems; (3) quarterly feedback figures for FPs. Four other PTAM groups were matched controls. Primary outcome measure was the number of RTI-related antibiotic prescriptions after the intervention, assessed with multilevel linear regression analyses. Total number and number of prescriptions stratified by age (under/over 12 years) were analysed. At baseline, the average total number of RTI-related antibiotic prescriptions per 1,000 patients was 207.9 and 176.7 in the intervention and control PTAM groups, respectively. At follow-up, FPs in both the intervention and control groups prescribed significantly less antibiotics. For adolescents and adults, the drop in number of antibiotic prescription was significantly larger in the intervention groups (-27.8 per 1,000 patients) than the control groups (-7.2 per 1,000 patients; P<0.05). This multifaceted peer-group-based intervention was effective in reducing the number of RTI-related antibiotic prescriptions for adolescents and adults. To affect antibiotic prescribing in children other methods are needed.
Conflict of interest statement
JWLC is supported by a Veni-grant (91614078) of the Netherlands Organisation for Health Research and Development (ZonMw). LvD received unrestricted grants from Astra Zeneca, BMS and Pfizer for research not related to this study. MV, MAM, ME and LSvdH declare no potential conflicts of interest.
Figures
References
-
- Levy, S. B. Antibiotic resistance-the problem intensifies. Adv. Drug Deliv. Rev. 57, 1446–1450 (2005). - PubMed
-
- Livermore, D. M. Bacterial resistance: origins, epidemiology, and impact. Clin. Infect. Dis. 36, S11–S23 (2003). - PubMed
-
- ECDC/EMEA. The Bacterial Challenge: Time to React. A Call to Narrow the Gap Between Multidrug-Resistant Bacteria in the EU and the Development of New Antibacterial. Agents ECDC/EMEA joint technical report (Stockholm, 2009).
-
- Smucny, J. , Fahey, T. , Becker, L. , Glazier, R. & McIsaac, W. Antibiotics for acute bronchitis. Cochrane Database Syst. Rev. 2000, CD000245 (2000). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
