

Review
doi: 10.1259/bjr.20150672.
Epub 2016 Feb 5.
Extragenital endometriosis: assessment with MR imaging. A pictorial review
Affiliations
- PMID: 26846303
- PMCID: PMC4846200
- DOI: 10.1259/bjr.20150672
Item in Clipboard
Review
Extragenital endometriosis: assessment with MR imaging. A pictorial review
Br J Radiol.
2016.
Abstract
Endometriosis is a gynaecologic disease characterized by endometrial tissue outside the uterine cavity. Commonly it affects the pelvic organs. When endometrial nodules or plaques are localized in sites other than the uterus or ovaries, it is termed extragenital endometriosis. Adequate pre-operative assessment is essential for treatment planning. MRI is a non-invasive method with high spatial resolution that allows the multiplanar evaluation of genital and extragenital endometriosis. Herein, we present a pictorial review of a variety of extragenital endometriosis cases, all of which can be encountered in clinical practice.
Figures
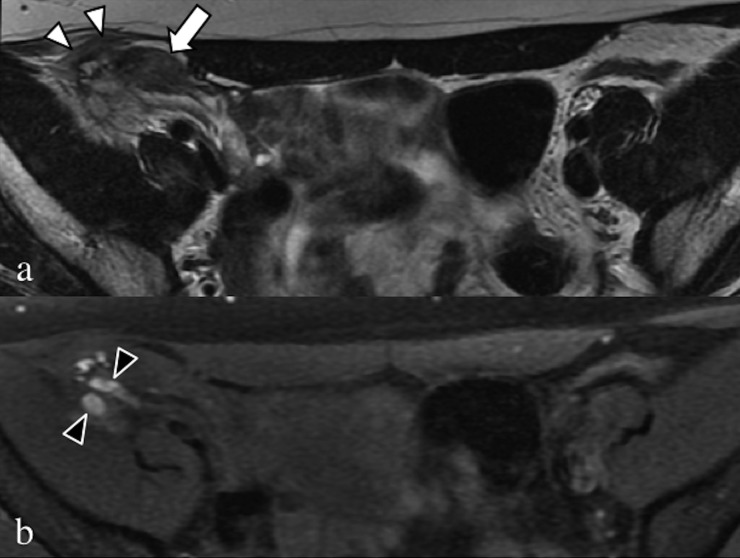
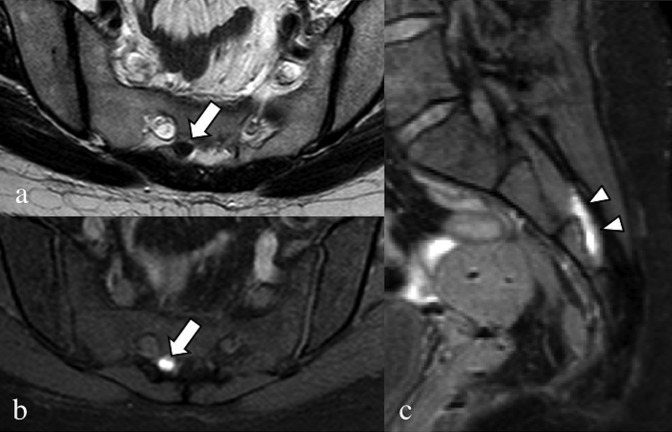
Axial T2 weighted (a) and fat-saturated T1 weighted (b) images. Large fibrotic and haemorrhagic endometrial localization (arrow) in the middle and lateral portion of the right round ligament infiltrating the oblique muscle and the T1 weighted sequence (black arrowheads).
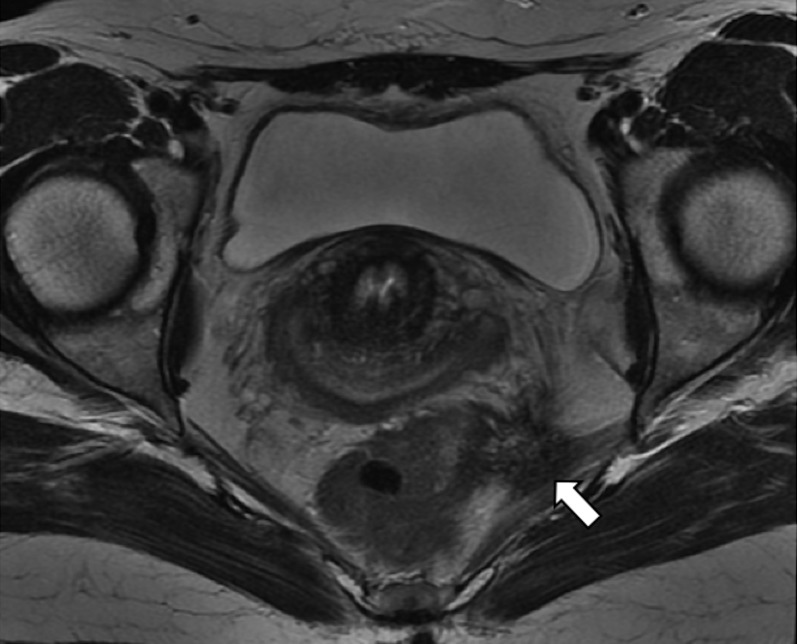
Axial T2 weighted image. Retracting endometrial lesion (arrows) of the left uterosacral ligament, with involvement of the piriformis muscle and the lateral wall of the rectus.
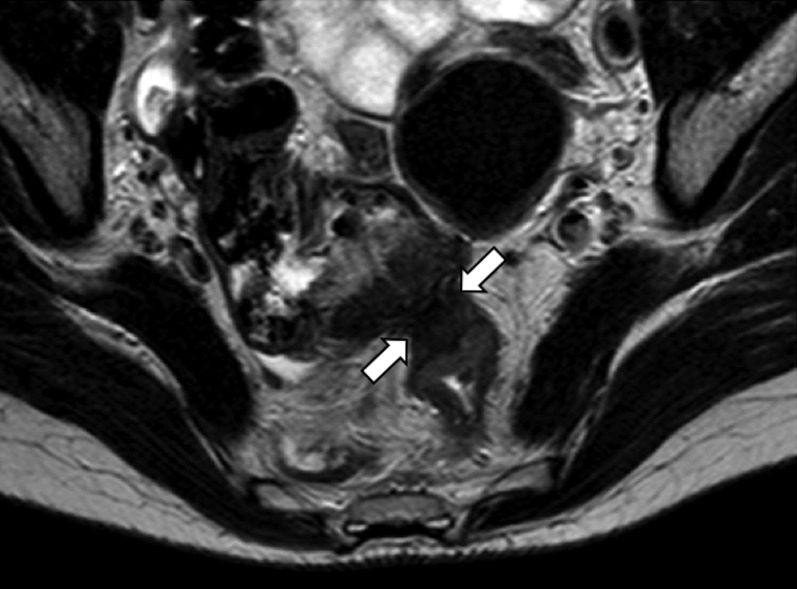
Axial T2 weighted image. Hypointense endometrial lesion (arrows), with invasion and retraction of the anterior wall of the left colon and of the caecum wall, which is dislocated in the Douglas' pouch. The fat plane is obscured.
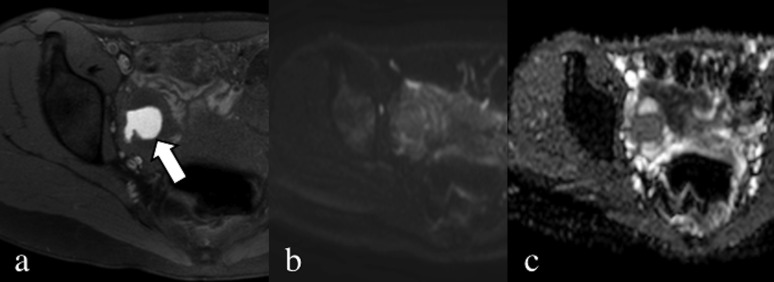
Axial fat-saturated T1 weighted image without contrast (a), diffusion-weighted image (b = 900) (b) and apparent diffusion coefficient map (c). Endometrial lesion of the right ovary characterized by the presence of blood (arrow); the mass has no specific slightly restricted diffusion water movement.
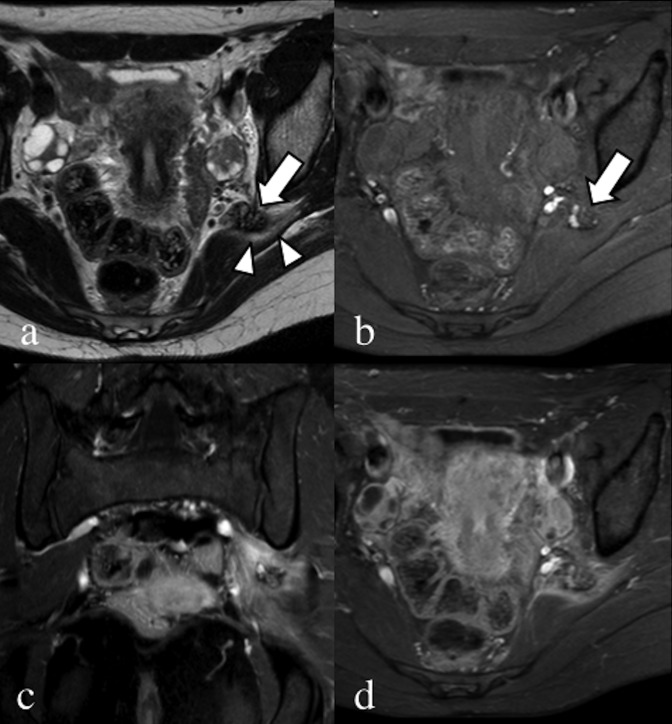
Axial T2 weighted (a) and fat-saturated pre-contrast T1 weighted (b) images. Coronal (c) and axial (d) fat-saturated T1 weighted images after the injection of gadolinium contrast media. A 28-year-old patient, with catamenial sciatic pain. Endometrial nodular lesion of the left sciatic nerve (arrows), characterized by hypointense signal with hyperintense foci on the T2 weighted image. Notice the oedema of the piriformis muscle (arrowheads). After contrast injection, there is enhancement of the piriformis muscle due to inflammation, clearly seen in the coronal image compared with the contralateral.
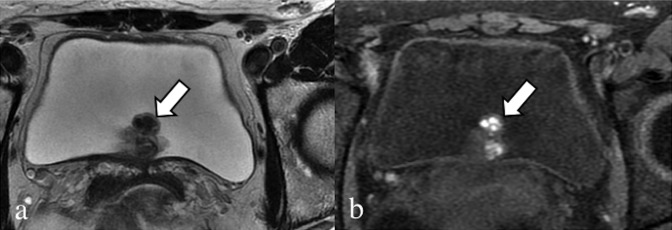
Axial T2 weighted (a) and fat-saturated T1 (b) weighted images. Exophytic endometrial lesion (arrows) of the posterior bladder wall, showing lobulated margins, low signal in T2 weighted image and very high signal blood foci in the T1 weighted image sequence.

Coronal fat-saturated T1 weighted image (a), sagittal (b) and coronal (c) T2 weighted images. Fibrotic and haemorrhagic endometrial nodule (arrows) in the abdominal wall affecting both rectus muscles, arising from the scar of the previous C-section.
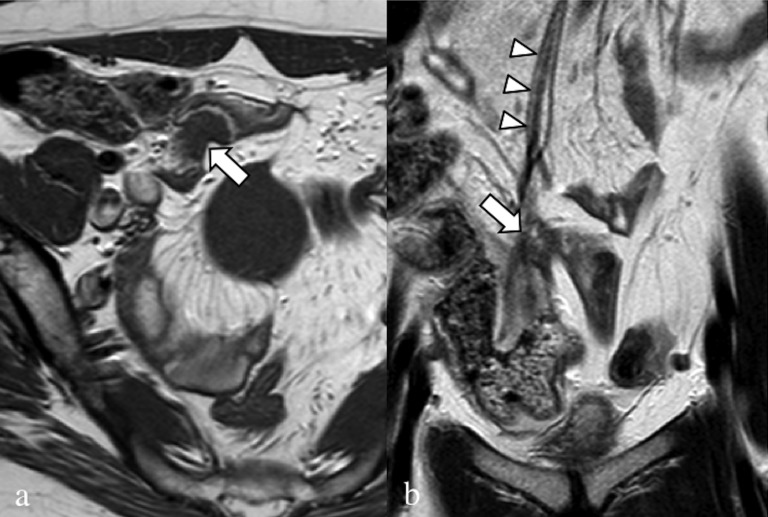
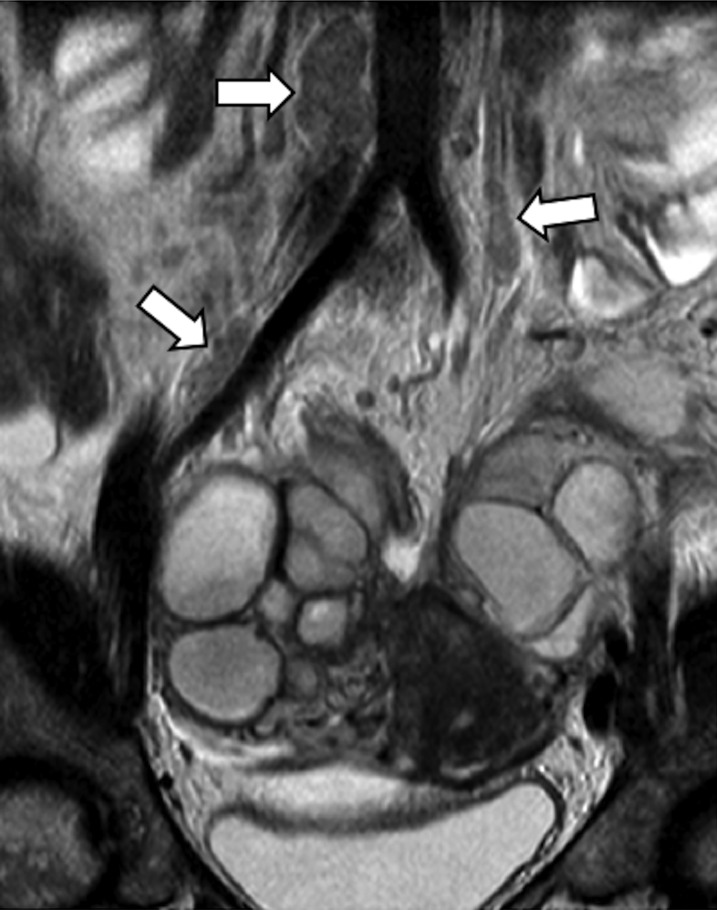
Axial (a) and coronal (b) T2 weighted images. Small bowel endometrial lesion (arrows), with hypointense signal. The lesion grows in the lumen of the bowel with partial obstruction. In the coronal view, the hypointense vertical lines (arrowheads) represent retracting fibrotic strands.
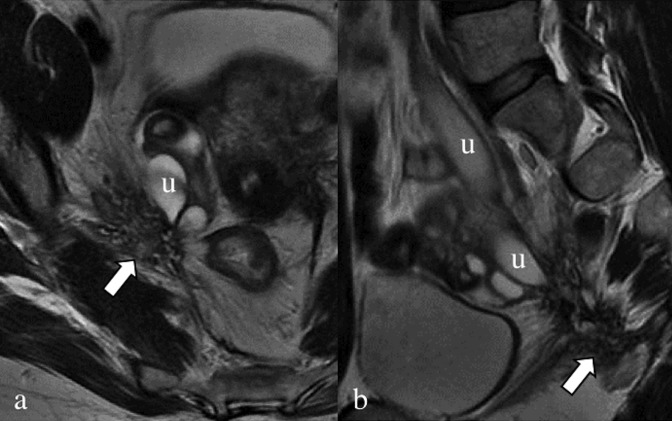
Axial (a) and sagittal (b) T2 weighted images. Retracting endometrial lesion (arrows), located in the lower portion of the right obturator region, anteriorly to the piriformis muscle. The nodule has a stellate shape with undefined margins, and the right ureter (u) is obstructed with consequent hydroureteronephrosis.
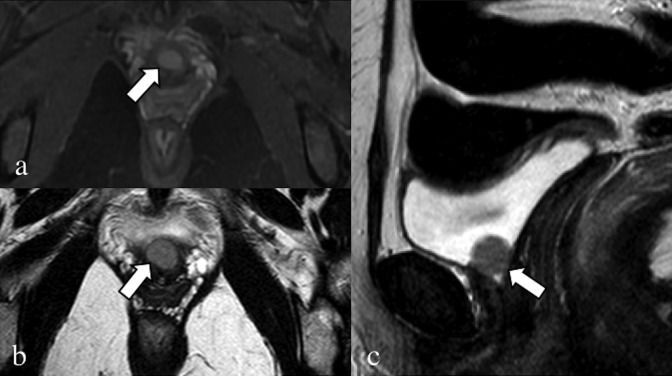
Axial fat-saturated T1 weighted image (a), axial (b) and sagittal (c) T2 weighted images. 45-year-old patient, operated for severe pelvic endometriosis (hysterectomy). Solid round-shaped lesion of the bladder neck-first segment of the urethra (arrows), showing high signal in the T1 weighted sequence and intermediate signal in the T2 weighted sequences.
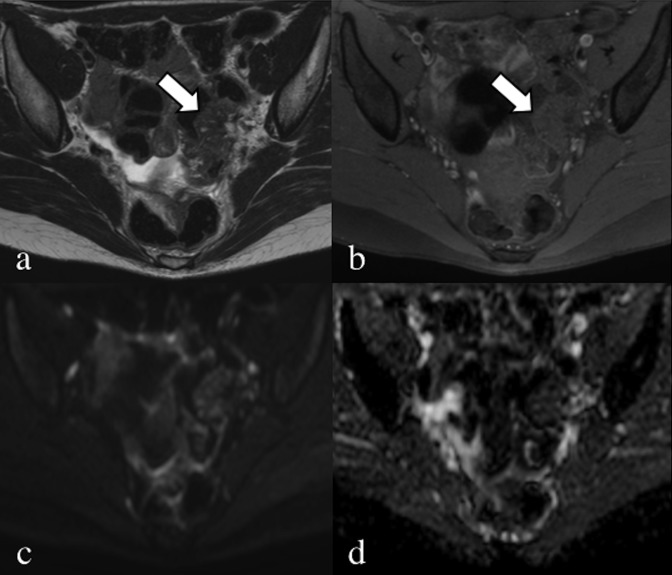
Axial T2 weighted (a) and fat-saturated T1 weighted images (b). A 33-year-old patient, with pelvic pain and catamenial haematochezia. Typical “mushroom cup” appearance (arrows) of a stenotic endometrial lesion of the sigma; the wall is irregularly thickened with hypointense signal and some hyperintense foci in the T2 weighted image. Diffusion-weighted image (b = 900) (c) and apparent diffusion coefficient map (d) showing a slightly restricted movement of water, not specific but consistent with an endometrial lesion as proved after surgery.
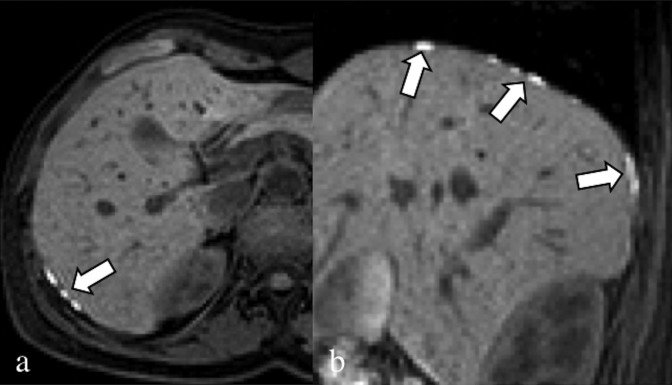
Axial (a) and sagittal (b) fat-saturated T1 weighted image. 30-year-old patient complaining about dysmenorrhoea and upper abdominal pain, which travelled to the right shoulder. Multiple endometrial lesions of the diaphragm (arrows); the nodules are characterized by a hyperintense signal in the fat-saturated T1 weighted sequences owing to the presence of blood.

Sagittal T2 weighted (a) and fat-saturated T1 weighted (b) images. A 29-year-old patient, with catamenial bleeding from the navel. Haemorrhagic endometrial lesion located at the navel (arrows). In the anterior wall of the uterus, there is a round-shaped hypointense subserosal fibroid.
Coronal T2 weighted image. A 35-year-old patient with chronic pelvic pain. Severe endometrial lesions of the ovaries. The MRI scan showed unspecific multiple lobulated lymph nodes >15 mm (arrows): based on the presence of endometriomas, an additional endometrial localization was supposed, but malignancies could not be excluded. After surgical removal, the lymph nodes proved positive for endometriosis.
Axial T2 weighted image (a), axial (b) and sagittal (c) fat-saturated T1 weighted images. A 32-year-old patient, operated on numerous times for severe pelvic endometriosis (hysterectomy); the patient complained about right catamenial claudication. In (a) and (b), the intracanal root of the right nerve S3 (arrows) is enlarged, with hypointense signal in the T2 weighted sequence and very high signal in the T1 weighted sequence. Even the extracanal portion of S3 (arrowheads) is enlarged with very high signal.
Similar articles
-
Beyond the boundaries-endometriosis: typical and atypical locations.Curr Probl Diagn Radiol. 2011 Nov-Dec;40(6):219-32. doi: 10.1067/j.cpradiol.2011.01.003. Curr Probl Diagn Radiol. 2011. PMID: 21939816
-
[Relevance of MRI for endometriosis diagnosis].Rofo. 2011 May;183(5):423-31. doi: 10.1055/s-0029-1245997. Epub 2011 Jan 18. Rofo. 2011. PMID: 21246473 Review. German.
-
[Magnetic resonance imaging in the diagnosis of different forms of endometriosis].Vestn Rentgenol Radiol. 2003 Jul-Aug;(4):45-59. Vestn Rentgenol Radiol. 2003. PMID: 14619398 Russian.
-
[Ureteric and bladder involvement of deep pelvic endometriosis. Value of multidisciplinary surgical management].Prog Urol. 2006 Nov;16(5):588-93. Prog Urol. 2006. PMID: 17175957 French.
-
Extragenital endometriosis--a clinicopathological review of a Glasgow hospital experience with case illustrations.J Obstet Gynaecol. 2004 Oct;24(7):804-8. doi: 10.1080/01443610400009568. J Obstet Gynaecol. 2004. PMID: 15763794 Review.
Cited by
-
Rectal endometriosis presenting as toxic megacolon.Autops Case Rep. 2021 Sep 3;11:e2021319. doi: 10.4322/acr.2021.319. eCollection 2021. Autops Case Rep. 2021. PMID: 34540725 Free PMC article.
-
Estrogen is essential but not sufficient to induce endometriosis.J Biosci. 2017 Jun;42(2):251-263. doi: 10.1007/s12038-017-9687-4. J Biosci. 2017. PMID: 28569249
-
Real world perspectives on endometriosis disease phenotyping through surgery, omics, health data, and artificial intelligence.NPJ Womens Health. 2025;3(1):8. doi: 10.1038/s44294-024-00052-w. Epub 2025 Feb 6. NPJ Womens Health. 2025. PMID: 39926583 Free PMC article. Review.
-
Advances in Imaging for Assessing Pelvic Endometriosis.Diagnostics (Basel). 2022 Nov 26;12(12):2960. doi: 10.3390/diagnostics12122960. Diagnostics (Basel). 2022. PMID: 36552967 Free PMC article. Review.
-
Therapeutic Potential of Natural Resources Against Endometriosis: Current Advances and Future Perspectives.Drug Des Devel Ther. 2024 Aug 21;18:3667-3696. doi: 10.2147/DDDT.S464910. eCollection 2024. Drug Des Devel Ther. 2024. PMID: 39188919 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
