

A randomised controlled trial of meloxicam, a Cox-2 inhibitor, to prevent hepatocellular carcinoma recurrence after initial curative treatment
- PMID: 26846471
- PMCID: PMC5003903
- DOI: 10.1007/s12072-016-9704-y
A randomised controlled trial of meloxicam, a Cox-2 inhibitor, to prevent hepatocellular carcinoma recurrence after initial curative treatment
Abstract
Background: Because the recurrence rate of hepatocellular carcinoma (HCC) is high, even after curative treatments such as hepatic resection and microwave ablation, chemopreventive agents that can effectively suppress HCC recurrence are required. Cyclooxygenase-2 (Cox-2) was recently found to be overexpressed in HCC. Therefore, Cox-2 inhibitors may offer a chemopreventive therapy for HCC. This randomised controlled trial (RCT) investigated the potential for meloxicam, a clinically used Cox-2 inhibitor, to prevent HCC recurrence after initial curative treatment.
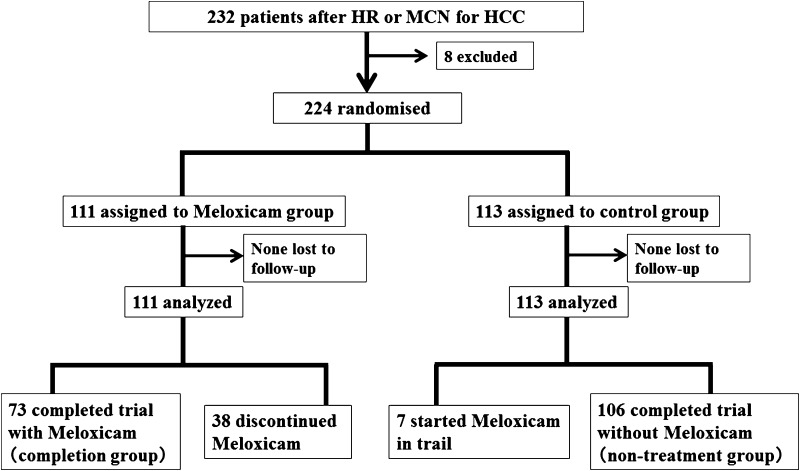
Methods: A total of 232 consecutive patients underwent hepatic resection and/or microwave ablation as initial therapy for HCC at our institute between July 2008 and April 2011. Eight patients were excluded because of poor renal function, history of non-steroidal anti-inflammatory drug-related ulceration, or multiple cancers. The remaining 224 patients were randomised to a control group (n = 113) or a meloxicam group (n = 111). To patients in the meloxicam group, meloxicam was administered at 15 mg daily (5 mg three times a day) as long as possible. The overall survival (OS) and disease-free survival (DFS) rates were determined.
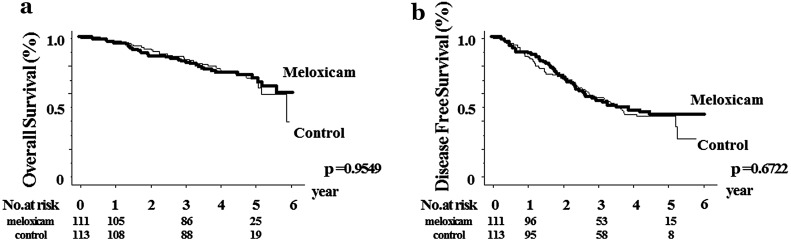
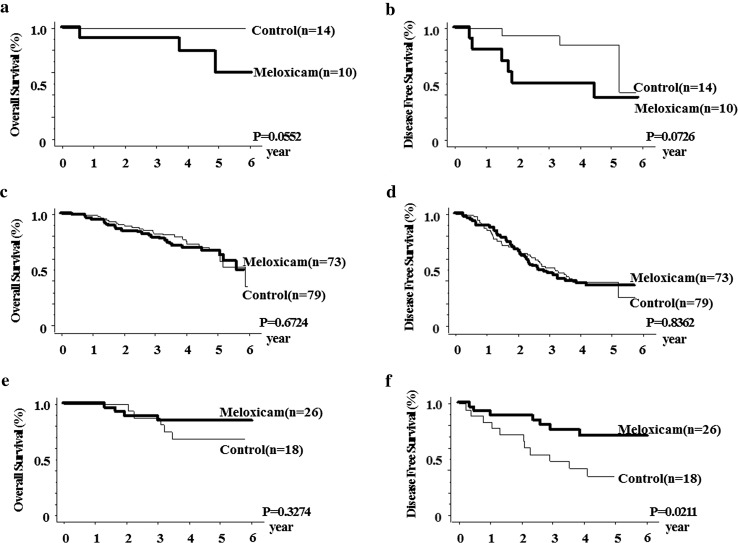
Results: The 1-, 3-, and 5-year OS rates of the meloxicam group were 95.4, 82.4, and 70.1 %, respectively. Those of the control group were 98.2, 85.1, and 71.5 %, respectively (p = 0.9549). The corresponding DFS rates of the meloxicam group were 89.2, 53.9, and 44.0 % and those of control group were 86.5, 57.0, and 43.4 %, respectively (p = 0.6722). In the OS and DFS of subsets including patients with hepatitis B or C virus infection, we could not find significant differences between the meloxicam and control groups. However, in the subgroup of analysis of patients without viral hepatitis (NBNC-HCC), significant differences were observed in the DFS between the meloxicam group (1-year DFS, 92.3 %; 3-year DFS, 75.8 %; 5-year DFS, 70.4 %) and control group (1-year DFS, 83.3 %; 3-year DFS, 48.1 %; 5-year DFS, not obtained) (p = 0.0211).
Conclusion: Administration of the Cox-2 inhibitor meloxicam may have a possibility to suppress HCC recurrence after initial curative treatments in patients with NBNC-HCC.
Keywords: Chemoprevention; Cox-2 inhibitor; Hepatocellular carcinoma; Recurrence.
Conflict of interest statement
Yuko Takami, Susumu Eguchi, Masaki Tateishi, Tomoki Ryu, Kazuhiro Mikagi, Yoshiyuki Wada, and Hideki Saitsu declare that they have no conflicts of interest. Ethical approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent Informed consent was obtained from all individual participants included in the study.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
