

The role of inflammation in the pathology of preeclampsia
- PMID: 26846579
- PMCID: PMC5484393
- DOI: 10.1042/CS20150702
The role of inflammation in the pathology of preeclampsia
Abstract
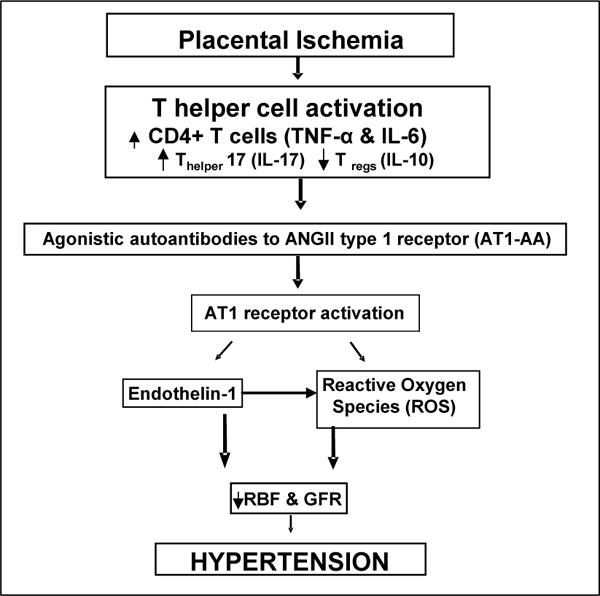
Preeclampsia (PE) affects 5-7% of all pregnancies in the United States and is the leading cause of maternal and prenatal morbidity. PE is associated with hypertension after week 20 of gestation, decreased renal function and small-for-gestational-age babies. Women with PE exhibit chronic inflammation and production of autoantibodies. It is hypothesized that during PE, placental ischaemia occurs as a result of shallow trophoblast invasion which is associated with an immune imbalance where pro-inflammatory CD4(+) T-cells are increased and T regulatory cells (Tregs) are decreased. This imbalance leads to chronic inflammation characterized by oxidative stress, pro-inflammatory cytokines and autoantibodies. Studies conducted in our laboratory have demonstrated the importance of this immune imbalance in causing hypertension in response to placental ischaemia in pregnant rats. These studies confirm that increased CD4(+) T-cells and decreased Tregs during pregnancy leads to elevated inflammatory cytokines, endothelin (ET-1), reactive oxygen species (ROS) and agonistic autoantibodies to the angiotensin II (Ang II), type 1 receptor (AT1-AA). All of these factors taken together play an important role in increasing the blood pressure during pregnancy. Specifically, this review focuses on the decrease in Tregs, and their associated regulatory cytokine interleukin (IL)-10, which is seen in response to placental ischaemia during pregnancy. This study will also examine the effect of regulatory immune cell repopulation on the pathophysiology of PE. These studies show that restoring the balance of the immune system through increasing Tregs, either by adoptive transfer or by infusing IL-10, reduces the blood pressure and pathophysiology associated with placental ischaemia in pregnant rats.
Keywords: hypertension; inflammation; pregnancy.
© 2016 Authors; published by Portland Press Limited.
Figures
References
-
- NHBPEP. Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. American journal of obstetrics and gynecology. 2000;183(1):S1–S22. Epub 2000/08/02. - PubMed
-
- Noris M, Perico N, Remuzzi G. Mechanisms of disease: Pre-eclampsia. Nature clinical practice Nephrology. 2005;1(2):98–114. quiz 20. Epub 2006/08/26. - PubMed
-
- Keyes LE, Armaza JF, Niermeyer S, Vargas E, Young DA, Moore LG. Intrauterine growth restriction, preeclampsia, and intrauterine mortality at high altitude in Bolivia. Pediatr Res. 2003;54(1):20–5. Epub 2003/04/18. - PubMed
-
- Lachmeijer AM, Arngrimsson R, Bastiaans EJ, Frigge ML, Pals G, Sigurdardottir S, et al. A genome-wide scan for preeclampsia in the Netherlands. Eur J Hum Genet. 2001;9(10):758–64. Epub 2002/01/10. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous