

Association of Slopes of Estimated Glomerular Filtration Rate With Post-End-Stage Renal Disease Mortality in Patients With Advanced Chronic Kidney Disease Transitioning to Dialysis
- PMID: 26848002
- PMCID: PMC4748393
- DOI: 10.1016/j.mayocp.2015.10.026
Association of Slopes of Estimated Glomerular Filtration Rate With Post-End-Stage Renal Disease Mortality in Patients With Advanced Chronic Kidney Disease Transitioning to Dialysis
Abstract
Objective: To investigate the association of estimated glomerular filtration rate (eGFR) slopes before dialysis initiation with cause-specific mortality after dialysis initiation.
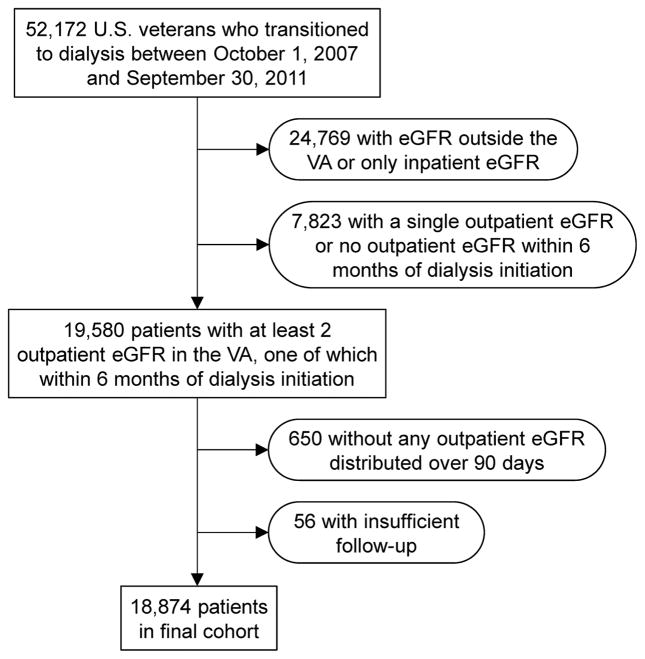
Patients and methods: In this retrospective cohort study of 18,874 US veterans who had transitioned to dialysis from October 1, 2007, through September 30, 2011, we examined the association of pre-end-stage renal disease (ESRD) eGFR slopes with all-cause, cardiovascular, and infection-related mortality during the post-ESRD period over a median follow-up of 2.0 years (interquartile range, 1.1-3.2 years). Associations were examined using Cox models with adjustment for potential confounders.
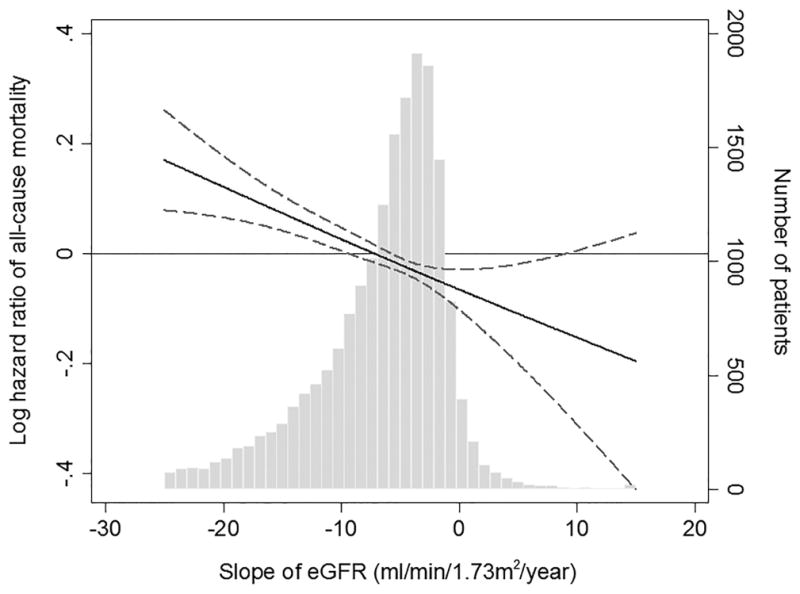
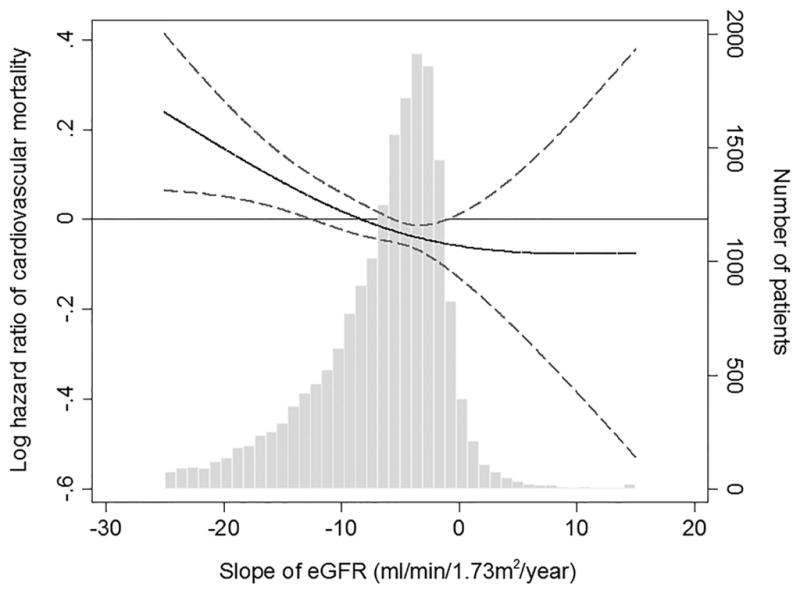
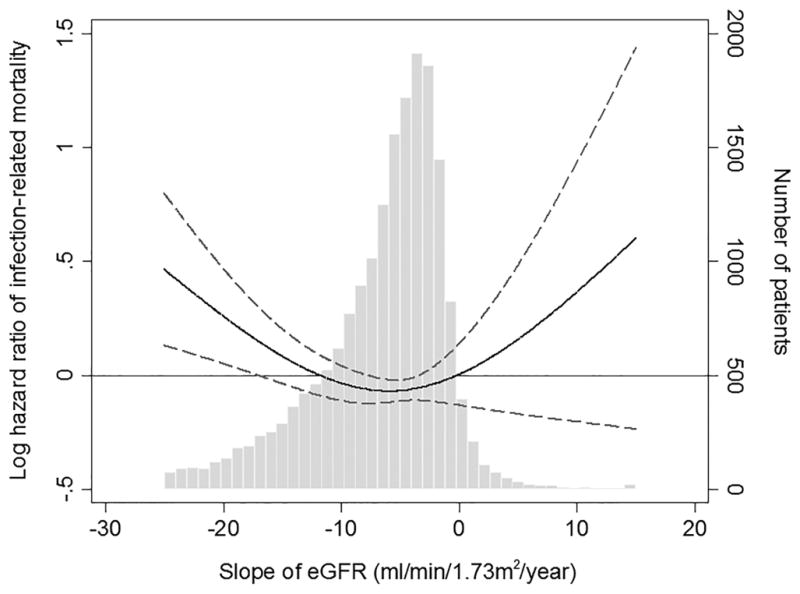
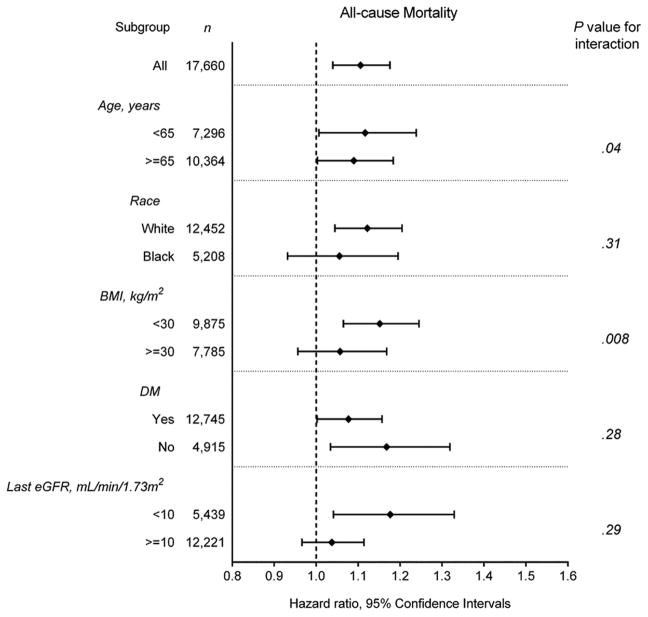
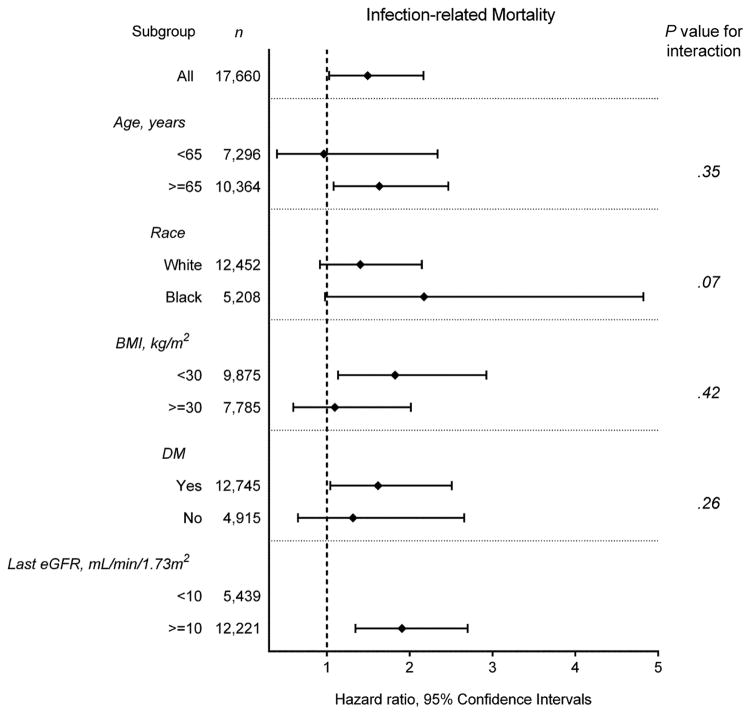
Results: Before the 18,874 patients transitioned to dialysis, 4485 (23.8%), 5633 (29.8%), and 7942 (42.1%) experienced fast, moderate, and slow eGFR decline, respectively, and 814 (4.3%) had increasing eGFR (defined as eGFR slopes of less than -10, -10 to less than -5, -5 to <0, and ≥0 mL/min per 1.73 m(2) per year). During the study period, a total of 9744 all-cause, 2702 cardiovascular, and 604 infection-related deaths were observed. Compared with patients with slow eGFR decline, those with moderate and fast eGFR decline had a higher risk of all-cause mortality (adjusted hazard ratio [HR], 1.06; 95% CI, 1.00-1.11; and HR, 1.11; 95% CI, 1.04-1.18, respectively) and cardiovascular mortality (HR, 1.11; 95% CI, 1.01-1.23 and HR, 1.13; 95% CI, 1.00-1.27, respectively). In contrast, increasing eGFR was only associated with higher infection-related mortality (HR, 1.49; 95% CI, 1.03-2.17).
Conclusion: Rapid eGFR decline is associated with higher all-cause and cardiovascular mortality, and increasing eGFR is associated with higher infection-related mortality among incident dialysis cases.
Copyright © 2016 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
None.
Figures

Similar articles
-
Prognostic significance of pre-end-stage renal disease serum alkaline phosphatase for post-end-stage renal disease mortality in late-stage chronic kidney disease patients transitioning to dialysis.Nephrol Dial Transplant. 2018 Feb 1;33(2):264-273. doi: 10.1093/ndt/gfw412. Nephrol Dial Transplant. 2018. PMID: 28064159 Free PMC article.
-
Predialysis Kidney Function and Its Rate of Decline Predict Mortality and Hospitalizations After Starting Dialysis.Mayo Clin Proc. 2018 Aug;93(8):1074-1085. doi: 10.1016/j.mayocp.2018.01.030. Epub 2018 Jul 4. Mayo Clin Proc. 2018. PMID: 30078411 Free PMC article.
-
Primary causes of kidney disease and mortality in dialysis-dependent children.Pediatr Nephrol. 2020 May;35(5):851-860. doi: 10.1007/s00467-019-04457-7. Epub 2020 Feb 4. Pediatr Nephrol. 2020. PMID: 32020338 Free PMC article.
-
Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without hypertension: a meta-analysis.Lancet. 2012 Nov 10;380(9854):1649-61. doi: 10.1016/S0140-6736(12)61272-0. Epub 2012 Sep 24. Lancet. 2012. PMID: 23013600 Free PMC article. Review.
-
Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: a meta-analysis.Lancet. 2012 Nov 10;380(9854):1662-73. doi: 10.1016/S0140-6736(12)61350-6. Epub 2012 Sep 24. Lancet. 2012. PMID: 23013602 Free PMC article. Review.
Cited by
-
Association between vascular access creation and deceleration of estimated glomerular filtration rate decline in late-stage chronic kidney disease patients transitioning to end-stage renal disease.Nephrol Dial Transplant. 2017 Aug 1;32(8):1330-1337. doi: 10.1093/ndt/gfw220. Nephrol Dial Transplant. 2017. PMID: 27242372 Free PMC article.
-
Blood Pressure Before Initiation of Maintenance Dialysis and Subsequent Mortality.Am J Kidney Dis. 2017 Aug;70(2):207-217. doi: 10.1053/j.ajkd.2016.12.020. Epub 2017 Mar 11. Am J Kidney Dis. 2017. PMID: 28291617 Free PMC article.
-
Laxative use in patients with advanced chronic kidney disease transitioning to dialysis.Nephrol Dial Transplant. 2021 Nov 9;36(11):2018-2026. doi: 10.1093/ndt/gfaa205. Nephrol Dial Transplant. 2021. PMID: 33035325 Free PMC article.
-
Early Mortality Associated with Inpatient versus Outpatient Hemodialysis Initiation in a Large Cohort of US Veterans with Incident End-Stage Renal Disease.Nephron. 2017;137(1):15-22. doi: 10.1159/000473704. Epub 2017 Apr 27. Nephron. 2017. PMID: 28445893 Free PMC article.
-
Association between renal function and cardiovascular mortality: a retrospective cohort study of elderly from health check-up.BMJ Open. 2021 Sep 21;11(9):e049307. doi: 10.1136/bmjopen-2021-049307. BMJ Open. 2021. PMID: 34548356 Free PMC article.
References
-
- United States Renal Data System. 2014 Annual Data Report: Epidemiology of Kidney Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda, MD: 2014.
-
- Bradbury BD, Fissell RB, Albert JM, et al. Predictors of early mortality among incident US hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS) Clin J Am Soc Nephrol. 2007;2(1):89–99. - PubMed
-
- Turin TC, Coresh J, Tonelli M, et al. Short-term change in kidney function and risk of end-stage renal disease. Nephrol Dial Transplant. 2012;27(10):3835–3843. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
