

Anomalous origin of the coronary artery arising from the opposite sinus: prevalence and outcomes in patients undergoing coronary CTA
- PMID: 26848152
- PMCID: PMC6279103
- DOI: 10.1093/ehjci/jev323
Anomalous origin of the coronary artery arising from the opposite sinus: prevalence and outcomes in patients undergoing coronary CTA
Abstract
Aims: The impact of coronary computed tomographic angiography (CTA) on management of anomalous origin of the coronary artery arising from the opposite sinus (ACAOS) remains uncertain. We examined the prevalence, anatomical characterization, and outcomes of ACAOS patients undergoing CTA.
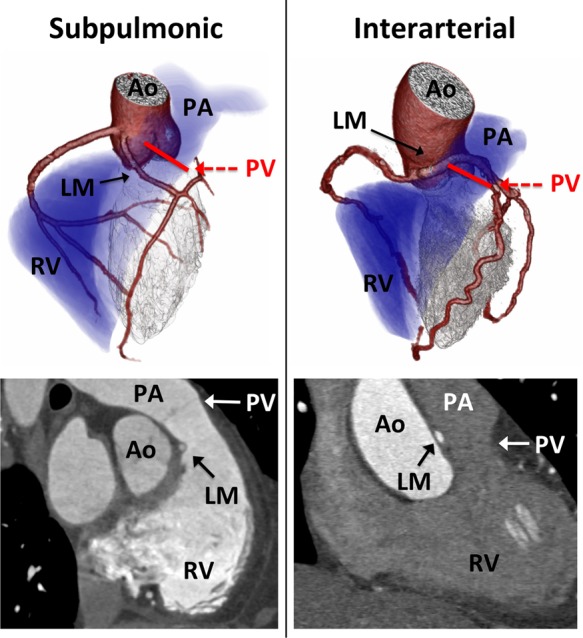
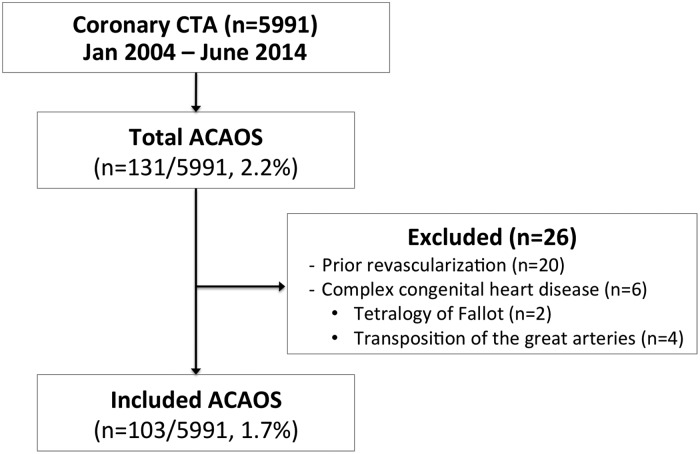
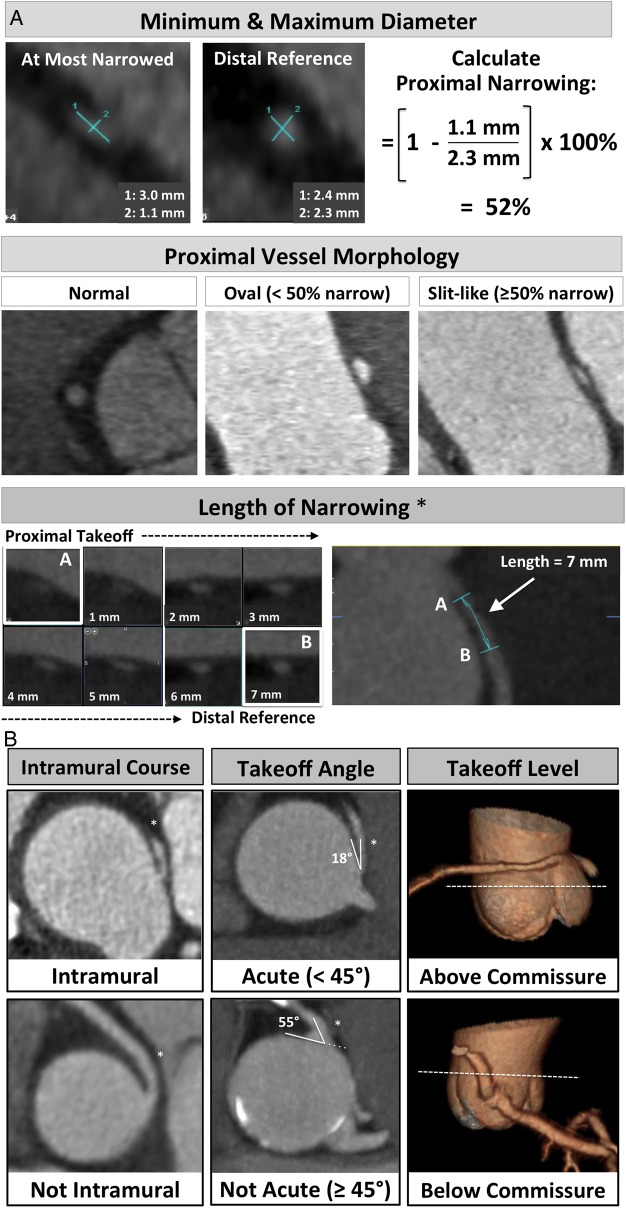
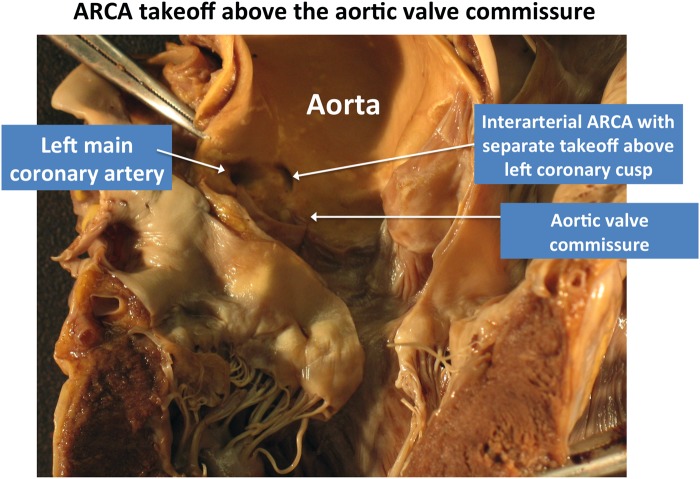
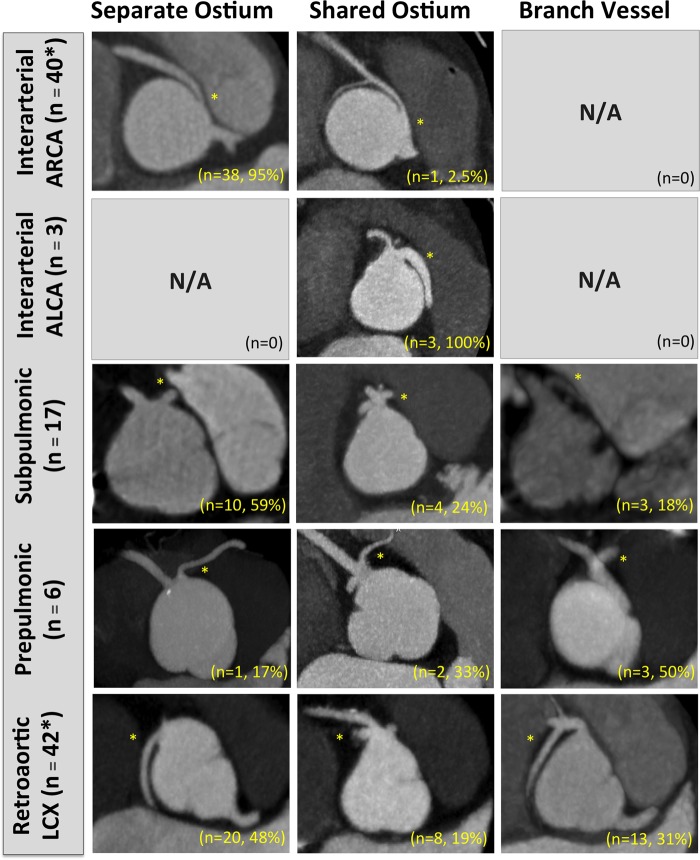
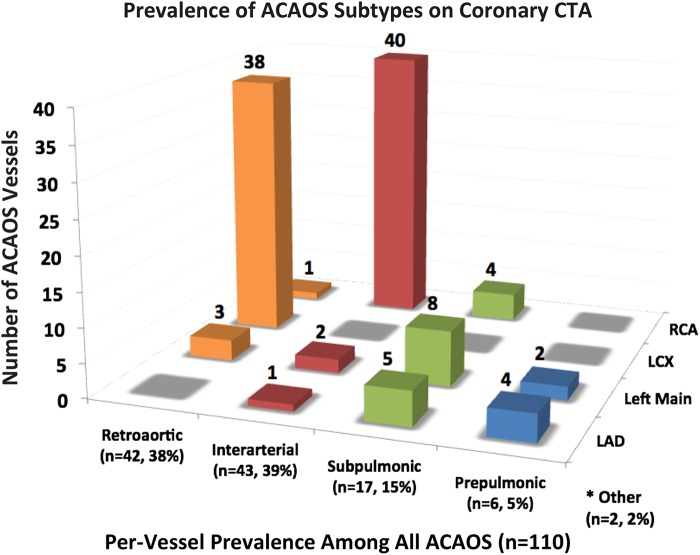
Methods and results: Among 5991 patients referred for CTA at two tertiary hospitals between January 2004 and June 2014, we identified 103 patients (1.7% prevalence) with 110 ACAOS vessels. Mean age was 52 years (range 5-83, 63% male), with 55% previously known ACAOS and 45% discovered on CTA. ACAOS subtypes included: 39% interarterial (n = 40 anomalous right coronary artery, n = 3 anomalous left coronary artery), 38% retroaortic, 15% subpulmonic, 5% prepulmonic, and 2% other. ACAOS patients were assessed for symptoms, ischaemic test results, revascularization, all-cause or cardiovascular (CV) death, and myocardial infarction. CTAs were reviewed for ACAOS course, take-off height and angle, length and severity of proximal narrowing, intramural course, and obstructive coronary artery disease (CAD). In follow-up (median 5.8 years), there were 20 surgical revascularizations and 3 CV deaths. After adjusting for obstructive CAD (n = 21/103, 20%), variables associated with ACAOS revascularization included the following: CV symptoms, proximal vessel narrowing ≥50%, length of narrowing >5.4 mm, and an interarterial course.
Conclusion: The prevalence of ACAOS on CTA was 1.7%, including 45% of cases discovered incidentally. CTA provided excellent characterization of ACAOS features associated with coronary revascularization, including the length and severity of proximal vessel narrowing.
Keywords: anomalous coronary artery; coronary computed tomographic angiography; prognosis; revascularization; sudden cardiac death.
Published by Oxford University Press on behalf of the European Society of Cardiology 2016. This work is written by US Government employees and is in the public domain in the US.
Figures

References
-
- Warnes CA, Williams RG, Bashore TM, Child JS, Connolly HM, Dearani JA et al. . ACC/AHA 2008 guidelines for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults With Congenital Heart Disease). Developed in Collaboration With the American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol 2008;52:e143–263. - PubMed
-
- Dodd JD, Ferencik M, Liberthson RR, Cury RC, Hoffmann U, Brady TJ et al. . Congenital anomalies of coronary artery origin in adults: 64-MDCT appearance. Am J Roentgenol 2007;188:W138–46. - PubMed
-
- Bittencourt MS, Hulten E, Ghoshhajra B, O'Leary D, Christman MP, Montana P et al. . Prognostic value of nonobstructive and obstructive coronary artery disease detected by coronary computed tomography angiography to identify cardiovascular events. Circ Cardiovasc Imaging 2014;7:282–91. - PubMed
-
- Maron BJ, Ackerman MJ, Nishimura RA, Pyeritz RE, Towbin JA, Udelson JE. Task Force 4: HCM and other cardiomyopathies, mitral valve prolapse, myocarditis, and Marfan syndrome. J Am Coll Cardiol 2005;45:1340–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
