

Visual intraoperative estimation of cup and stem position is not reliable in minimally invasive hip arthroplasty
- PMID: 26848628
- PMCID: PMC4900086
- DOI: 10.3109/17453674.2015.1137182
Visual intraoperative estimation of cup and stem position is not reliable in minimally invasive hip arthroplasty
Abstract
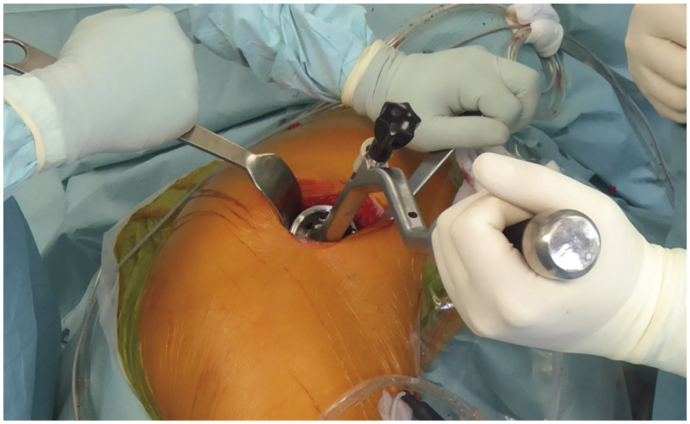
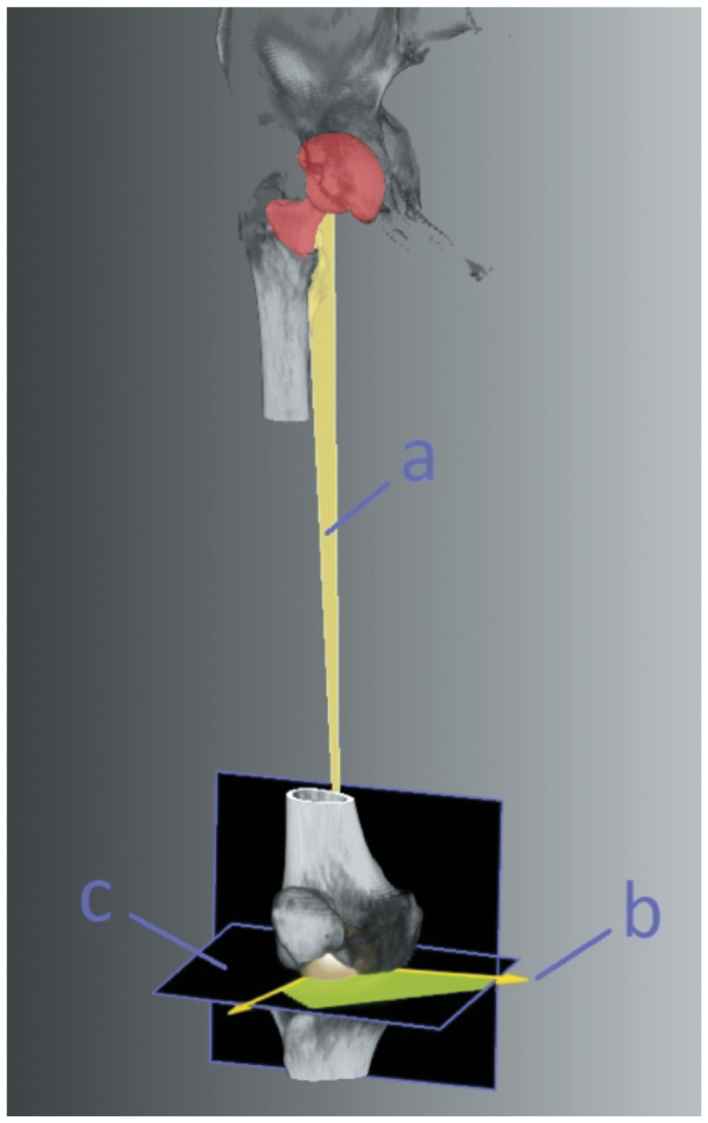
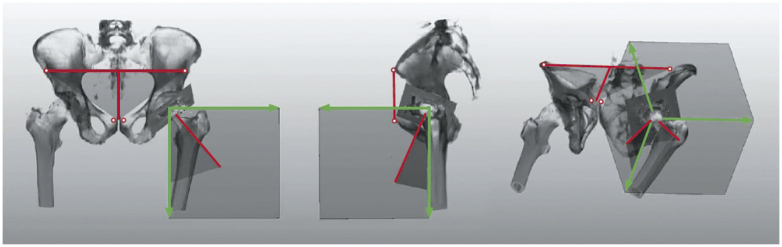
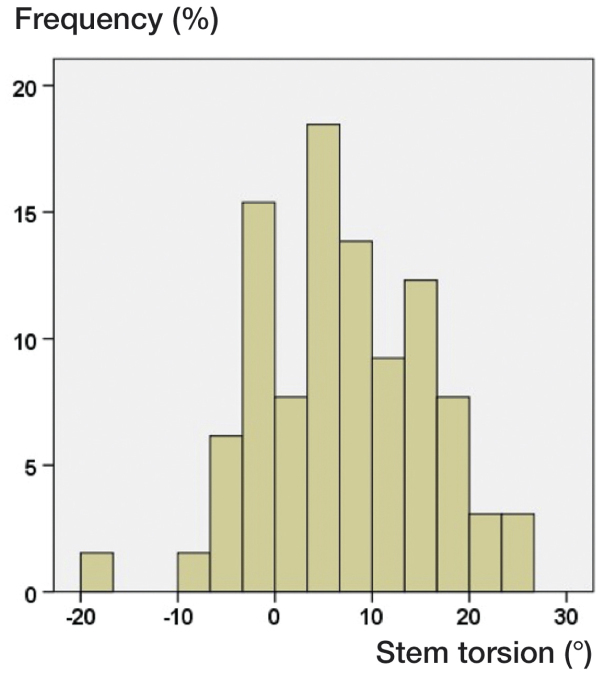
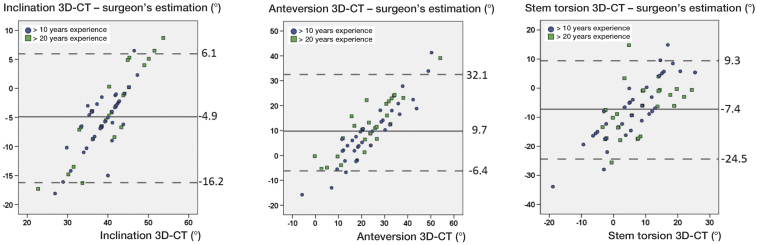
Background and purpose - In hip arthroplasty, acetabular inclination and anteversion-and also femoral stem torsion-are generally assessed by eye intraoperatively. We assessed whether visual estimation of cup and stem position is reliable. Patients and methods - In the course of a subgroup analysis of a prospective clinical trial, 65 patients underwent cementless hip arthroplasty using a minimally invasive anterolateral approach in lateral decubitus position. Altogether, 4 experienced surgeons assessed cup position intraoperatively according to the operative definition by Murray in the anterior pelvic plane and stem torsion in relation to the femoral condylar plane. Inclination, anteversion, and stem torsion were measured blind postoperatively on 3D-CT and compared to intraoperative results. Results - The mean difference between the 3D-CT results and intraoperative estimations by eye was -4.9° (-18 to 8.7) for inclination, 9.7° (-16 to 41) for anteversion, and -7.3° (-34 to 15) for stem torsion. We found an overestimation of > 5° for cup inclination in 32 hips, an overestimation of > 5° for stem torsion in 40 hips, and an underestimation < 5° for cup anteversion in 42 hips. The level of professional experience and patient characteristics had no clinically relevant effect on the accuracy of estimation by eye. Altogether, 46 stems were located outside the native norm of 10-20° as defined by Tönnis, measured on 3D-CT. Interpretation - Even an experienced surgeon's intraoperative estimation of cup and stem position by eye is not reliable compared to 3D-CT in minimally invasive THA. The use of mechanical insertion jigs, intraoperative fluoroscopy, or imageless navigation is recommended for correct implant insertion.
Figures
Comment on
-
Dislocations after total hip-replacement arthroplasties.J Bone Joint Surg Am. 1978 Mar;60(2):217-20. J Bone Joint Surg Am. 1978. PMID: 641088
-
Anterior iliopsoas impingement after total hip arthroplasty.J Arthroplasty. 1995 Aug;10(4):546-9. doi: 10.1016/s0883-5403(05)80160-3. J Arthroplasty. 1995. PMID: 8523018
-
Pelvic tilt makes acetabular cup navigation inaccurate.Acta Orthop. 2005 Aug;76(4):517-23. doi: 10.1080/17453670510041501. Acta Orthop. 2005. PMID: 16195068
-
Functional pelvic orientation measured from lateral standing and sitting radiographs.Clin Orthop Relat Res. 2006 Dec;453:272-6. doi: 10.1097/01.blo.0000238862.92356.45. Clin Orthop Relat Res. 2006. PMID: 17006364
-
Impingement with total hip replacement.J Bone Joint Surg Am. 2007 Aug;89(8):1832-42. doi: 10.2106/JBJS.F.01313. J Bone Joint Surg Am. 2007. PMID: 17671025 Review.
-
Medium- and long-term performance of 11,516 uncemented primary femoral stems from the Norwegian arthroplasty register.J Bone Joint Surg Br. 2007 Dec;89(12):1574-80. doi: 10.1302/0301-620X.89B12.18969. J Bone Joint Surg Br. 2007. PMID: 18057355
-
The influence of acetabular component position on wear in total hip arthroplasty.J Arthroplasty. 2008 Jan;23(1):51-6. doi: 10.1016/j.arth.2007.06.008. J Arthroplasty. 2008. PMID: 18165028
-
Combined anteversion technique for total hip arthroplasty.Clin Orthop Relat Res. 2009 Jan;467(1):119-27. doi: 10.1007/s11999-008-0598-4. Epub 2008 Nov 1. Clin Orthop Relat Res. 2009. PMID: 18979146 Free PMC article. Clinical Trial.
-
Femoral anteversion in THA and its lack of correlation with native acetabular anteversion.Clin Orthop Relat Res. 2010 Feb;468(2):527-32. doi: 10.1007/s11999-009-1040-2. Epub 2009 Aug 28. Clin Orthop Relat Res. 2010. PMID: 19714389 Free PMC article.
-
A comparison of surgeon estimation and computed tomographic measurement of femoral component anteversion in cementless total hip arthroplasty.J Bone Joint Surg Am. 2009 Nov;91(11):2598-604. doi: 10.2106/JBJS.H.01225. J Bone Joint Surg Am. 2009. PMID: 19884433
-
Stem torsion in total hip replacement.Acta Orthop. 2010 Oct;81(5):579-82. doi: 10.3109/17453674.2010.524596. Acta Orthop. 2010. PMID: 20919811 Free PMC article.
-
Research synthesis of recommended acetabular cup orientations for total hip arthroplasty.J Arthroplasty. 2014 Feb;29(2):377-82. doi: 10.1016/j.arth.2013.06.026. Epub 2013 Aug 17. J Arthroplasty. 2014. PMID: 23958234
-
[Complications after minimally invasive total hip arthroplasty].Orthopade. 2014 Jan;43(1):47-53. doi: 10.1007/s00132-013-2123-z. Orthopade. 2014. PMID: 24362903 German.
-
Is the acetabular cup orientation after total hip arthroplasty on a two dimension or three dimension model accurate?Int Orthop. 2014 Oct;38(10):2009-15. doi: 10.1007/s00264-014-2336-8. Epub 2014 Apr 16. Int Orthop. 2014. PMID: 24737148
-
[Influence of surgeon experience in total hip arthroplasty. Dependence on operating time and complication risk].Orthopade. 2014 Jun;43(6):522-8. doi: 10.1007/s00132-014-2292-4. Orthopade. 2014. PMID: 24816976 German.
-
Fixation and wear with a contemporary acetabular component and cross-linked polyethylene at minimum 10-year follow-up.J Arthroplasty. 2014 Oct;29(10):1961-9. doi: 10.1016/j.arth.2014.05.008. Epub 2014 May 15. J Arthroplasty. 2014. PMID: 24939638
-
The relationship between operative and radiographic acetabular component orientation: which factors influence resultant cup orientation?Bone Joint J. 2014 Oct;96-B(10):1290-7. doi: 10.1302/0301-620X.96B10.34100. Bone Joint J. 2014. PMID: 25274911
-
Impingement-free range of movement, acetabular component cover and early clinical results comparing 'femur-first' navigation and 'conventional' minimally invasive total hip arthroplasty: a randomised controlled trial.Bone Joint J. 2015 Jul;97-B(7):890-8. doi: 10.1302/0301-620X.97B7.34729. Bone Joint J. 2015. PMID: 26130342 Clinical Trial.
References
-
- Barrack R. Dislocation after total hip arthroplasty: implant design and orientation. J Am Acad Orthop Surg 2003; 11: 89–99. - PubMed
-
- Bedard N, Callaghan J, Stefl M, Williams T, Liu S, Goetz D.. Fixation and wear with contemporary acetabular components and cross-linked polyethylene at 10-year follow-up. J Arthroplasty 2014; 29: 1961–9. - PubMed
-
- Craiovan B, Renkawitz T, Weber M, Grifka J, Nolte L, Zheng G.. Is the acetabular cup orientation after total hip arthroplasty on a two dimension or three dimension model accurate? Int Orthop 2014; 38(10): 2009–15. - PubMed
-
- DiGioia A, Hafez M, Jaramaz B, Levison T, Moody J.. Functional pelvic orientation measured from lateral standing and sitting radiographs. Clin Orthop Relat Res 2006; 453: 272–276. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical