

Adjusted Age-Adjusted Charlson Comorbidity Index Score as a Risk Measure of Perioperative Mortality before Cancer Surgery
- PMID: 26848761
- PMCID: PMC4744039
- DOI: 10.1371/journal.pone.0148076
Adjusted Age-Adjusted Charlson Comorbidity Index Score as a Risk Measure of Perioperative Mortality before Cancer Surgery
Erratum in
-
Correction: Adjusted Age-Adjusted Charlson Comorbidity Index Score as a Risk Measure of Perioperative Mortality before Cancer Surgery.PLoS One. 2016 Jun 15;11(6):e0157900. doi: 10.1371/journal.pone.0157900. eCollection 2016. PLoS One. 2016. PMID: 27303810 Free PMC article.
Abstract
Background: Identification of patients at risk of death from cancer surgery should aid in preoperative preparation. The purpose of this study is to assess and adjust the age-adjusted Charlson comorbidity index (ACCI) to identify cancer patients with increased risk of perioperative mortality.
Methods: We identified 156,151 patients undergoing surgery for one of the ten common cancers between 2007 and 2011 in the Taiwan National Health Insurance Research Database. Half of the patients were randomly selected, and a multivariate logistic regression analysis was used to develop an adjusted-ACCI score for estimating the risk of 90-day mortality by variables from the original ACCI. The score was validated. The association between the score and perioperative mortality was analyzed.
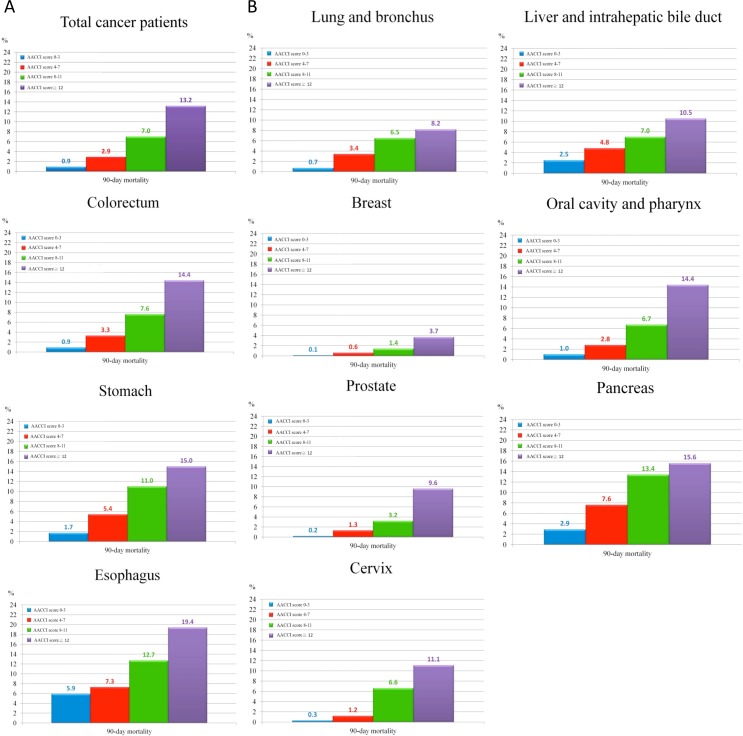
Results: The adjusted-ACCI score yield a better discrimination on mortality after cancer surgery than the original ACCI score, with c-statics of 0.75 versus 0.71. Over 80 years of age, 70-80 years, and renal disease had the strongest impact on mortality, hazard ratios 8.40, 3.63, and 3.09 (P < 0.001), respectively. The overall 90-day mortality rates in the entire cohort varied from 0.9%, 2.9%, 7.0%, and 13.2% in four risk groups stratifying by the adjusted-ACCI score; the adjusted hazard ratio for score 4-7, 8-11, and ≥ 12 was 2.84, 6.07, and 11.17 (P < 0.001), respectively, in 90-day mortality compared to score 0-3.
Conclusions: The adjusted-ACCI score helps to identify patients with a higher risk of 90-day mortality after cancer surgery. It might be particularly helpful for preoperative evaluation of patients over 80 years of age.
Conflict of interest statement
Figures
References
-
- World Health Organization, Cancer, Fact Sheet. http://www.who.int/mediacentre/factsheets/fs297/en/. Accessed Jan 20, 2015.
-
- Taiwan Cancer Registry. Five Years Survival of Cancers. http://tcr.cph.ntu.edu.tw/main.php?Page=A5B3. Accessed Jan 20, 2015.
-
- Mayr R, May M, Martini T, Lodde M, Comploj E, Pycha A, et al. Comorbidity and performance indices as predictors of cancer-independent mortality but not of cancer-specific mortality after radical cystectomy for urothelial carcinoma of the bladder. European urology. 2012;62(4):662–70. 10.1016/j.eururo.2012.03.057 . - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
