

Evaluation of the Therapeutic Potential of Anti-TLR4-Antibody MTS510 in Experimental Stroke and Significance of Different Routes of Application
- PMID: 26849209
- PMCID: PMC4746129
- DOI: 10.1371/journal.pone.0148428
Evaluation of the Therapeutic Potential of Anti-TLR4-Antibody MTS510 in Experimental Stroke and Significance of Different Routes of Application
Abstract
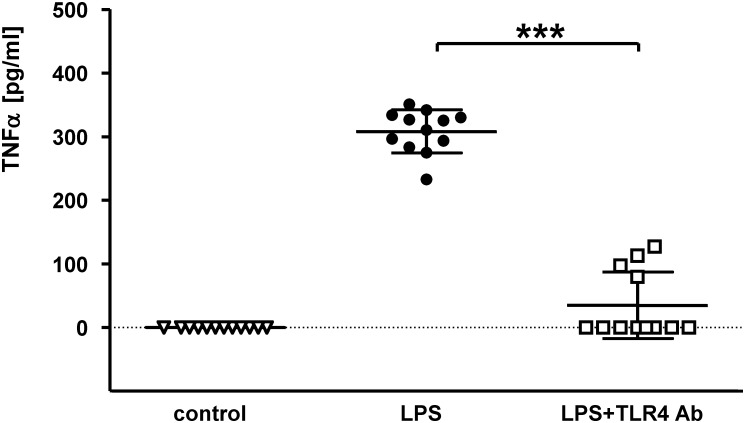
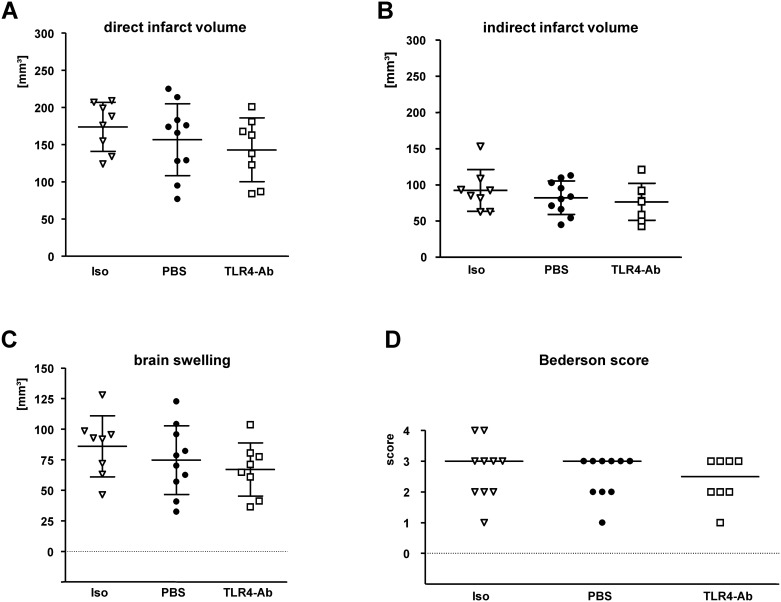
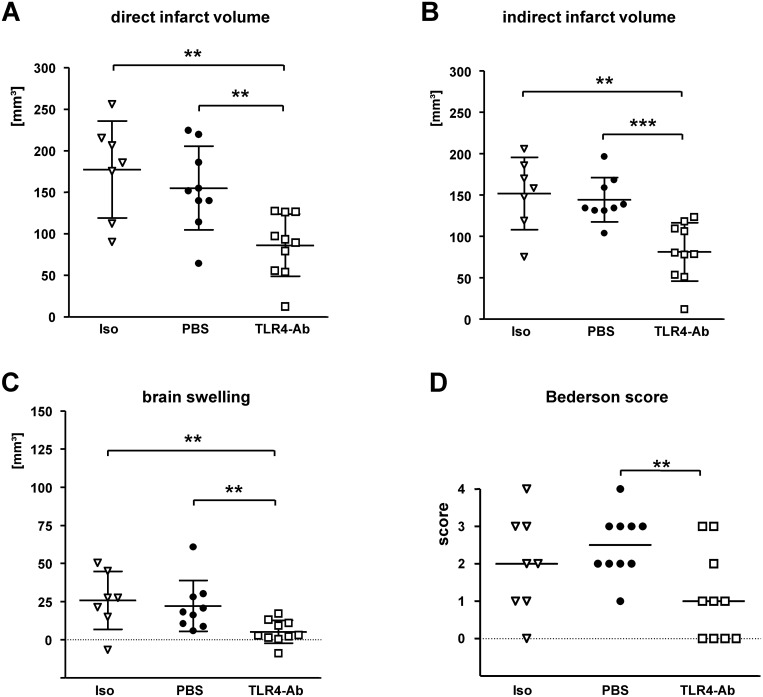
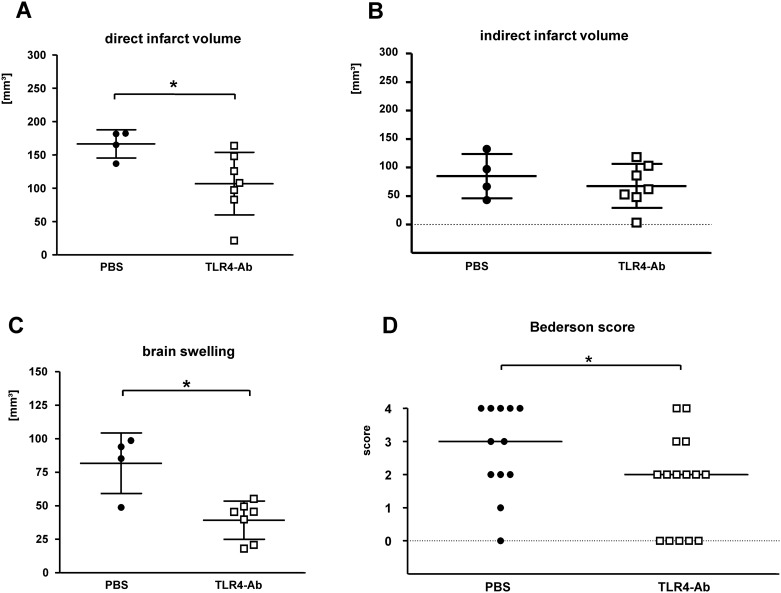
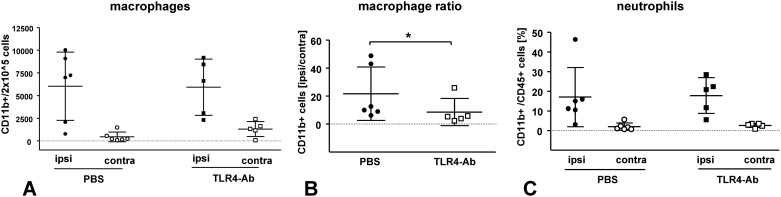
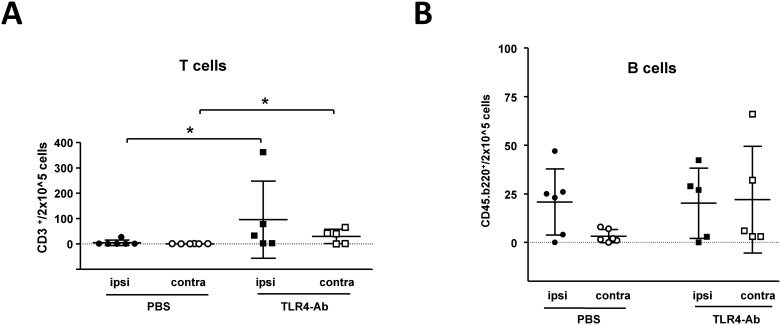
Toll-like receptors (TLRs) are central sensors for the inflammatory response in ischemia-reperfusion injury. We therefore investigated whether TLR4 inhibition could be used to treat stroke in a standard model of focal cerebral ischemia. Anti-TLR4/MD2-antibody (mAb clone MTS510) blocked TLR4-induced cell activation in vitro, as reported previously. Here, different routes of MTS510 application in vivo were used to study the effects on stroke outcome up to 2d after occlusion of the middle cerebral artery (MCAO) for 45 min in adult male C57Bl/6 wild-type mice. Improved neurological performance, reduced infarct volumes, and reduced brain swelling showed that intravascular application of MTS510 had a protective effect in the model of 45 min MCAO. Evaluation of potential long-term adverse effects of anti-TLR4-mAb-treament revealed no significant deleterious effect on infarct volumes nor neurological deficit after 14d of reperfusion in a mild model of stroke (15 min MCAO). Interestingly, inhibition of TLR4 resulted in an altered adaptive immune response at 48 hours after reperfusion. We conclude that blocking TLR4 by the use of specific mAb is a promising strategy for stroke therapy. However, long-term studies with increased functional sensitivity, larger sampling sizes and use of other species are required before a clinical use could be envisaged.
Conflict of interest statement
Figures
References
-
- Dirnagl U, Iadecola C, Moskowitz MA. Pathobiology of ischaemic stroke: an integrated view. Trends Neurosci 1999; 22: 391–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
