

The Burden of Provider-Initiated Preterm Birth and Associated Factors: Evidence from the Brazilian Multicenter Study on Preterm Birth (EMIP)
- PMID: 26849228
- PMCID: PMC4743970
- DOI: 10.1371/journal.pone.0148244
The Burden of Provider-Initiated Preterm Birth and Associated Factors: Evidence from the Brazilian Multicenter Study on Preterm Birth (EMIP)
Abstract
Background: About 15 million children are born under 37 weeks of gestation worldwide. Prematurity is the leading cause of neonatal deaths and short/long term morbidities, entailing consequences not only for the individual, but also their family, health agencies, facilities and all community. The provider-initiated preterm birth is currently one of the most important obstetric conditions related to preterm births, particularly in middle and high income countries, thus decreasing the need for therapeutic preterm birth is essential to reduce global prematurity. Therefore detailed knowledge on the factors associated with provider-initiated preterm birth is essential for the efforts to reduce preterm birth rates and its consequences. In this current analysis we aimed to assess the proportion of provider-initiated (pi-PTB) among preterm births in Brazil and identify associated factors.
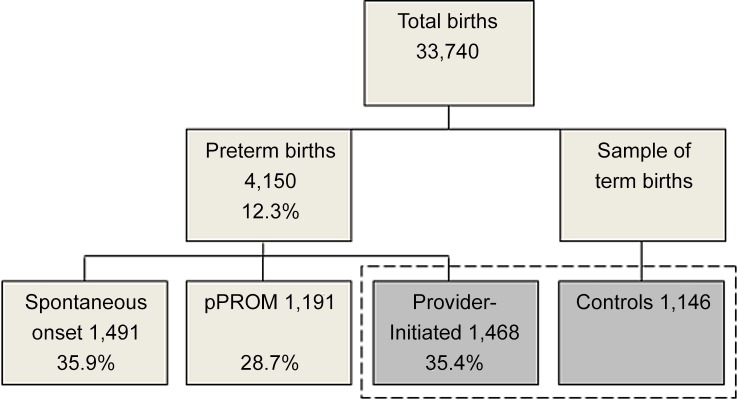
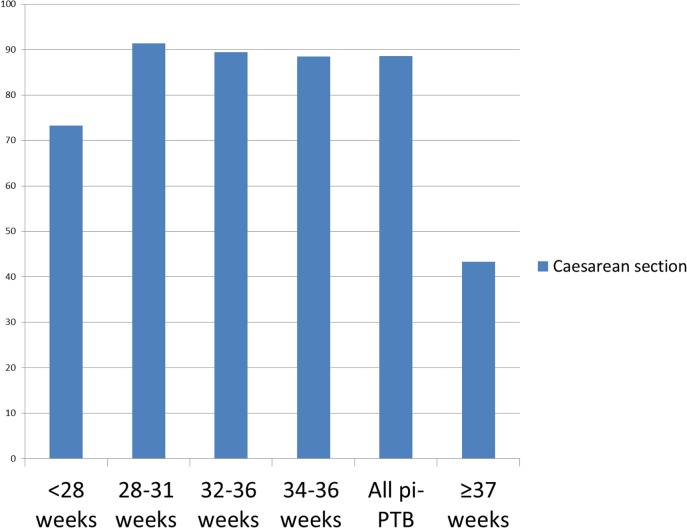
Methods and findings: This is an analysis of a multicenter cross-sectional study with a nested case-control component called Brazilian Multicenter Study on Preterm Birth (EMIP). EMIP was conducted in 20 referral obstetric hospitals located in the three most populated of the five Brazilian regions. We analysed data of women with pi-PTB, defined as childbirth occurring at less than 37 weeks, medically indicated for maternal/fetal compromise or both; and women with term birth, childbirth at or after 37 weeks. Maternal, sociodemographic, obstetric, prenatal care, delivery, and postnatal characteristics were assessed as possible factors associated with pi-PTB, compared to term births. The overall prevalence of preterm births was 12.3%. Of these, approximately one-third of cases were initiated by the provider. Hypertensive disorders, placental abruption, and diabetes were the main maternal conditions leading to pi-PTB. Caesarean section was the most common mode of delivery. Chronic hypertension (OR 7.47; 95%CI 4.02-13.88), preeclampsia/eclampsia/HELLP syndrome (OR 15.35; 6.57-35.88), multiple pregnancy (OR 12.49; 4.86-32.05), and chronic diabetes (OR 5.24; 2.68-10.25) were the most significant factors independently associated with pi-PTB.
Conclusions: pi-PTB is responsible for about one-third of all preterm births, requiring special attention. The decision-making process relative to the choice of provider-initiated birth is complex, and many factors should be elucidated to improve strategies for its prevention, including evidence-based guidelines on proper management of the corresponding clinical conditions.
Conflict of interest statement
Figures
References
-
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, et al. (2012) National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet 379(9832): 2162–72. 10.1016/S0140-6736(12)60820-4 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
