

Risk Factors for Long-Term Mortality after Hospitalization for Community-Acquired Pneumonia: A 5-Year Prospective Follow-Up Study
- PMID: 26849359
- PMCID: PMC4746118
- DOI: 10.1371/journal.pone.0148741
Risk Factors for Long-Term Mortality after Hospitalization for Community-Acquired Pneumonia: A 5-Year Prospective Follow-Up Study
Abstract
Background: Contributors to long-term mortality in patients with community-acquired pneumonia (CAP) remain unclear, with little attention paid to pneumonia etiology. We examined long-term survival, causes of death, and risk factors for long-term mortality in adult patients who had been hospitalized for CAP, with emphasis on demographic, clinical, laboratory, and microbiological characteristics.
Methods: Two hundred and sixty-seven consecutive patients admitted in 2008-2011 to a general hospital with CAP were prospectively recruited and followed up. Patients who died during hospital stay were excluded. Demographic, clinical, and laboratory data were collected within 48 hours of admission. Extensive microbiological work-up was performed to establish the etiology of CAP in 63% of patients. Mortality data were obtained from the Norwegian Cause of Death Registry. Cox regression models were used to identify independent risk factors for all-cause mortality.
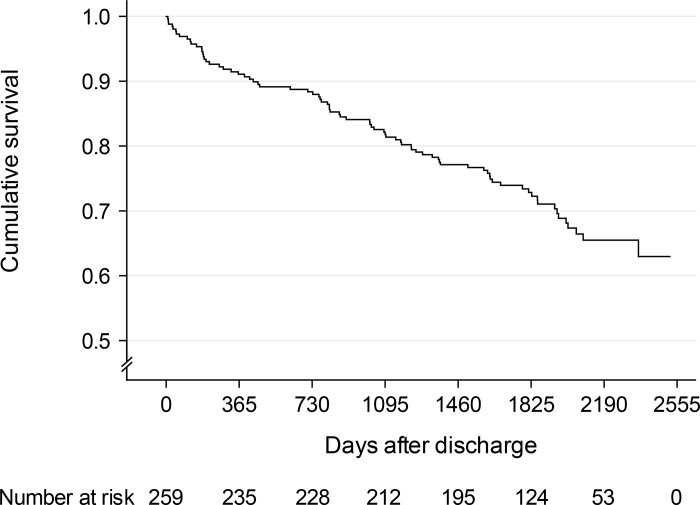
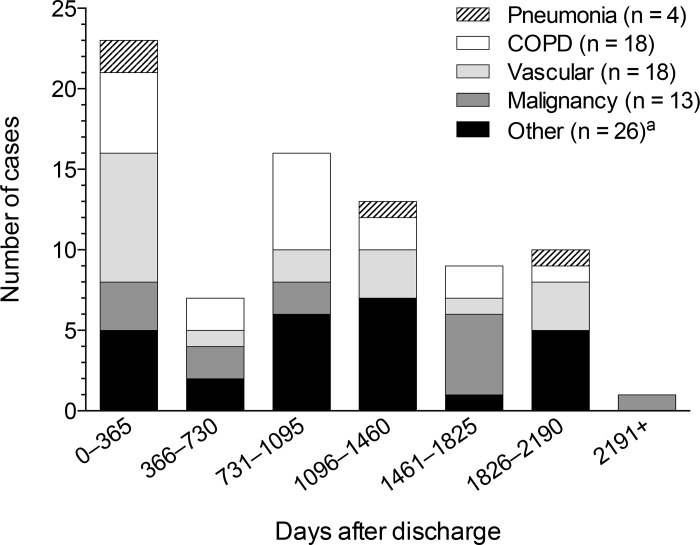
Results: Of 259 hospital survivors of CAP (median age 66 years), 79 (30.5%) died over a median of 1,804 days (range 1-2,520 days). Cumulative 5-year survival rate was 72.9% (95% CI 67.4-78.4%). Standardized mortality ratio was 2.90 for men and 2.05 for women. The main causes of death were chronic obstructive pulmonary disease (COPD), vascular diseases, and malignancy. Independent risk factors for death were the following (hazard ratio, 95% CI): age (1.83 per decade, 1.47-2.28), cardiovascular disease (2.63, 1.61-4.32), COPD (2.09, 1.27-3.45), immunocompromization (1.98, 1.17-3.37), and low serum albumin level at admission (0.75 per 5 g/L higher, 0.58-0.96), whereas active smoking was protective (0.32, 0.14-0.74); active smokers were younger than non-smokers (P < 0.001). Microbial etiology did not predict mortality.
Conclusions: Results largely confirm substantial comorbidity-related 5-year mortality after hospitalization for CAP and the impact of several well-known risk factors for death, and extend previous findings on the prognostic value of serum albumin level at hospital admission. Pneumonia etiology had no prognostic value, but this remains to be substantiated by further studies using extensive diagnostic microbiological methods in the identification of causative agents of CAP.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
